![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
106 Cards in this Set
- Front
- Back
|
Epilepsy |
Chronic condition characterised by two or more unprovoked seizures |
|
|
Seizure |
Transient neurological dysfunction caused by excessive activity of cortical neurones=> alteration in behaviour or/and EEG changes |
|
|
Causes of provoked seizure |
Fever, metabolic, trauma |
|
|
Tonic clonic (grand mal) seizure s/s |
- Generalised - prodrome of unease or irritability hours to days before the episode - Tonic ictal phase: muscle rigidity - Clonic ictal phase: repetitive violent jerking of face and limbs, tongue biting, cyanosis, frothing, incontinence - Post ictal phase: flaccid limbs, extensor plantar reflexes, headache, confusion, aching muscles, sore tongue, amnesia, elevated serum ck lasting hours |
|
|
Absences seizure (Petit mal) |
Usually only in children, unresponsive for 5-10sec with arrest of activity, staring, blinking or eye rolling, non post ictal confusion - 3 Hz spike and slow wave activity on EEG |
|
|
Myoclonic seizures |
Sporadic contractions localised muscle groups of one or more extremities |
|
|
Atonic seizure |
Loss of muscle tone leading to a drop attack |
|
|
Most common cause late onset seizures (>50 yrs old) |
Stroke causes 50-80% |
|
|
Simple seizures definition |
Preserved level of conciousness |
|
|
Complex seizures s/s |
- Altered level of conciousness (may appear to be awake but with altered awareness) - Classic = automatisms eg. Chewing, swallowing, lip-smacking, scratching, fumbling, running, disrobing etc - Can also be other sensory disturbance (eg. Dysphasic, dysmnesic (deja vu), illusions, epigastric fullness |
|
|
Simple seizures s/s |
- Motor: postural, vocalising, forceful turning of eyes/head, focal muscle rigidity/jerking, Jacksonian march (spreads to adjacent muscle groups distal=>proximal) - Sensory: unusual sensations affecting vision, hearing, smell, taste or touch - Autonomic: epigastric discomfort, pallor, sweating, flushing, piloerection, pupillary dilation |
|
|
Investigations for seizure |
- CBE, electrolytes, fasting blood glucose, Ca, Mg, ESR, Cr, liver enzymes, CK, prolactin - Consider toxicology screen, ETOH level, Antiepileptic drug levels - CT/MRI if new seizure without known cause or known epileptic with new neurological s/s - LP if fever or meningismus - EEG |
|
|
Tx seizures |
- Avoid trigger - Meds indicated if: ≥2 unprovoked seizures, known organic brain disease, EEG with epileptiform activity, first episode of status epilepticus, abnormal neurological exam or findings on neuroimaging. - Consider surgery if focal and refractory - Education, driving ban etc |
|
|
Status epilepticus. Def, ix, tx, comps |
- Unremitting seizure >5 mins, or successive seizures without return to baseline state. - ix: electrolytes, Ca, Mg, PO4, glucose, CBE, toxicology screen, ETOH levels, Antiepileptic drug levels - Tx: ABCs, vitals, glucose, ECG, Nasal O2, IV normal saline, IV glucose, IV thiamine, ABGs if in resp distress, IV lorazepam=>Phenytoin=>phenobarbital - Comps: anoxia, cerebral ischaemia+oedema+permanent deficits, rhabdo+renal failure, aspiration pneumonia, death in 20% |
|
|
Ischaemic stroke mechanisms |
- Arterial thrombosis *Large vessel stenosis or occlusion of ICA, vertebral or Intracranial arteries. Mostly caused by atherosclerosis, dissection or vasculitis =>dec. blood flow beyond lesion (haemodynamic stroke) *Small vessel/lacunar: caused by chronic DM=>vessel wall thickening, dec luminal diametre (mainly small penetrating arteries: basal ganglia, internal capsule, thalamus) Cardioembolic *Embolus from cardiac source: AF, rheumatic valve disease, prosthetic valves, recent MI, fibrous/IE Systemic hypoperfusion (global cerebral ischaemia) *Usually 2o to cardiac failure(arrest, MI, arryth) * Mostly affects watershed areas |
|
|
Haemorrhagic stroke mechs |
Intracerebral haemorrhage *HTN most common: rupture of aneurysm *Most common sites: putamen, thalamus, cerebellum, pons *Other causes: trauma, amyloid angiopathy, Vasc malforms, vasculitis, cocaine/amphetamine use SAH |
|
|
Stroke syndromes ACA |
- Contralateral leg paresis - Sensory loss - Cognitive deficits (e.g. apathy, confusion, and poorjudgment) |
|
|
Stroke syndrome MCA |
1. Contralateral weakness and sensory loss of face and arm 2. Cortical sensory loss 3. May have contralateral homonymous hemianopia or quadrantanopia 4. if dominant (usually left) hemisphere: aphasia 5. if non-dominant (usually right) hemisphere: neglect 6. eye deviation towards the side of the lesion + away from the weak side |
|
|
Stroke syndrome PCA |
1. Contralateral hemianopia or quadrantanopia 2. Midbrain findings: CN III and IV palsy/pupillary changes, hemiparesis 3. thalamic findings: sensory loss, amnesia, decreased level of consciousness 4. if bilateral: cortical blindness or prosopagnosia 5. dyslexia and alexia (visual association cortex) |
|
|
Stroke syndrome basilar artery |
Locked in sydrome 1. quadriparesis 2. dysarthria 3. impaired eye movements |
|
|
Stroke syndrome PICA (lateral medullary) |
- Ipsilateral ataxia, ipsilateral Horner’s,ipsilateral facial sensory loss - Contralateral limb impairment of pain+ temperature sensation (spinothalamic) - Nystagmus, vertigo, nausea/vomiting, dysphagia, dysarthria, hiccups |
|
|
Haemorrhagic stroke s/s |
Headache, altered mental status, seizures, nausea and vomiting, and/or marked hypertension. - Focal neurological deficits - Hemiparesis - Aphasia |
|
|
RFs and aetiology haemorrhagic stroke |
RFs: - Advanced age - Hypertension (up to 60% of cases) - Previous history of stroke - Alcohol abuse - Use of illicit drugs (eg, cocaine, other sympathomimetic drugs) Causes: - Hypertension - Cerebral amyloidosis - Coagulopathies - Anticoagulant therapy - Thrombolytic therapy for acute myocardial infarction (MI) or acute ischemic stroke (can cause iatrogenic hemorrhagic transformation) - Arteriovenous malformation (AVM) - Aneurysms, and other vascular malformations (venous and cavernous angiomas) - Vasculitis - Intracranial neoplasm |
|
|
SAH mechanism |
SAH=>elevated ICP=> impairs cerebral autoregulation. + acute vasoconstriction, microvascular platelet aggregation, and loss of microvascular perfusion=>profound reduction in blood flow and cerebral ischaemia |
|
|
SAH s/s |
- 75% present with an acute severe headache - 25% will present with LOC ~20% have hx of a sudden milder headache several weeks before the acute event (sentinel bleed) - Neck stiffness/CN palsies 11% mortality - Delayed cerebral ischaemia (vasospasm) and rebleeding are the main causes of morbidity and mortality in patients who survive the initial bleed. - Vasospasm s/s: altered conscious state or increased neurological deficit, >72 hrs post haemorrhage. |
|
|
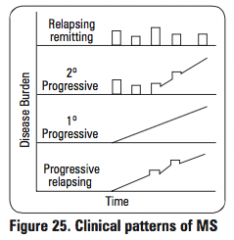
Patterns of MS |
|
|
|
Clinically isolated syndrome def |
Single MS like episode, may progress to MS |
|
|
MS definition |
2+ different attacks separated in space and time Space: One or more T2 bright lesions in: - periventricular - juxtacortical - infratentorial - spinal cord Time: - New lesion when compared to a previous scan - presence of asymptomatic enhancing lesion and a non-enhancing T2 bright lesion on any one scan |
|
|
Marburg (fulminant MS) |
Rapid progressive fatal MS, assoc w severe axonal damage, inflamm, necrosis |
|
|
Neuromyelitis optica |
Severe optic neuritis and extensive transverse myelitisextending >3 vertebral segments (NMO antibody positive) |
|
|
MS Aetiology |
Genetic: HLA-DRB1 Environmental *More common low sunlight areas (lower Vit D) * Linked to cetain viruses eg. EBV |
|
|
MS patho |
- CD4+ TH1 and TH17 T cells thatreact against self-myelin antigens&secrete cytokines => recruitleukocytes thatmediate damage=> secrete noxious inflammmediators=>myelin damage (plaque = infiltrate of Tcells and Mø)
- T cells pass through BBB and recognisemyelin basic proteins on as foreign=>release cytokines=> cytokines aretoxic to myelin, break down BBB and also recruit more immune cells => moreMø, T cells and B cells recruited&able to pass easily through damagedBBB=>activated B/T cells target myelin oligodendrocyte basic proteinw autoantibodies continuing myelin degradation. - Oligodendrocytes attempt torepair myelin=>over time repair mechanism become less effective=> reducedaxonal transport + sclerotic glial scars, potential axonal damage |
|
|
Venous stroke (intracranial venous thrombosis) |
- Thunderclap - Focal neuro deficits in region of vein |
|
|
Encephalitis RFs |
· Age<1 or >65 years · Immunodeficiency · viralinfections · blood/bodyfluid exposure · organtransplantation · animalor insect bites · location(exposure to different viruses typical of the area) · season(exposure to different viruses typical of the season) · swimmingor diving in warm freshwater · nasal/sinusirrigation (Naegleria) risk |
|
|
Encephalitis hx |
·Fever · Altered mental status · Photophobia · Headache · dec consciousness |
|
|
Encephalitis physical signs |
· Rash · Focal neurological deficits · Neck stiffness · Optic neuritis (ADEM) · s+s of the underlying virus (eg. Movement difficulties in CJD, parotitis in mumps, acute flaccid paralyisis in arboviruses and rabies, cough in influenza, HSV1 etc) · Seizures and status epilepticus (common in measles and HSV) · Loss of temperature and vasomotor control (dysautonomia) |
|
|
Ecephalitis pathogens |
- Identified in only 40-70% of cases - Viral (most comm) HSV, VZV, EBV, CMV, enteroviruses, West Nile, HIV, mumps, measles, rabies, polio - Bacteria: L. monocytogenes, Mycobacteria, spirochetes (Lyme, syphillis), Mycoplasma pneumoniae - Parasites: protozoa (e.g. Toxoplasma) - Fungi: e.g. Cryptococcus post-infectious (e.g. acute disseminated encephalomyelitis [ADEM]) auto-antibody mediated encephalitis anti-N-methyl-D-aspartate (NMDA) receptor encephalitis most commonin adults, most autoantibody-mediated encephalitis cases are associated with malignancy |
|
|
Red flags for headache |
- Onset >50 y/o or <10 (new/worse/different) (GCA, meningitis, tumours) - Unexplainable worsening or change of migraines - Sudden onset + extreme pain (thunderclap) - Sudden onset combined with rash, stiff neck, fever, lowering of consciousness, known sepsis (meningitis) - Worse on Valsalva, nausea, vomiting, waking up with headache, mood changes (inc. ICP) - New headache waking one up (haemorrhage, mass, cluster) - Fatigue, anorexia, night sweats, Hx cancer - Trauma - Pregnancy (preeclampsia, thrombosis) |
|
|
Normal pressure hydroceph def, s/s, Ix, tx |
- Wet, wobbly (ataxia, magnetic gait, often first sx), Weird (personality change, dementia, late finding, loss of spontaneity/initiative) Path: distortion of the central portion of the corona radiata by the distended ventricles. Periventricular white matter= sacral motor fibers=>legs/bladder - CT scan - Large volume LP (diagnostic and tx) - CSF shunting |
|
|
Hydroceph s/s |
Cognitive deterioration Headaches: prominent in morning dec absorption CSF when lying. Relieved by sitting headache becomes severe, continuous Neck pain: tonsilar herniation Nausea that is not exacerbated by head movements Vomiting: Sometimes explosive > in morning - Blurred vision + papilloedema optic nerve compromise - Horizontal diplopia from sixth nerve palsy - Difficulty in walking - Drowsiness - Incontinence (urinary first, fecal later). This indicates significant destruction of frontal lobes and advanced disease. |
|
|
Hydroceph tx |
- Decreasing CSF secretion by the choroid plexus w Acetazolamide (carbonic anhdrase inhib and furosemide) - LPs - Shunt |
|
|
Things that provoke seizures |
- Sleep deprivation - Excess alcohol - Illicit stimulant drugs - Antihistamines - Psychological stress - Some drugs eg bupropion, tramadol, pethidine - TCAs lower seizure threshold, use antipsychotics w caution - Abrupt cessation antiepileptics=>status epileptocus |
|
|
Cushing's reflex |
Inc. ICP=>ICP>MAP=>cerebral ischaemia=>activation of SNS&PNS=>SNS activation>PNS=>activation a-1 receptors=>vasoconstriction+tachycardia=>inc systemic BP in attempt to reperfuse brain. Stage 1 Baroreceptors in aortic arch detect inc BP=>PNS activation=>vagus nerve=>bradycardia (also caused by inc. ICP mechanically distorting vagus) But BP stays high to allow blood flow to brain |
|
|
Tension headache |
- Bilateral - Feeling of heaviness, pressure or tightness like a band around the head and down the neck |
|
|
Migraine definition epi |
>5 attacks, 4-72hrs duration + 2 of: *unilateral *pulsating *mod-severe *aggravated by physical act +1 of: *n/v *photo/phono/osmophobia 18% of women, 6% men (decreases w age, esp post-menopause) |
|
|
Migraine patho |
Not definitively known *depolarizing wave of “cortical spreading depression” across cerebral cortex=>aura *vasoconstriction/dilation significant * genetic contribution * triggers: stress, sleep excess/deprivation, drugs (oestrogen, nitroglycerin), hormonal changes, caffeine withdrawal, chocolate, tyramines, nitrites |
|
|
Approach to peripheral neuropathy |
1. differentiate: motor vs. sensory vs. autonomic vs. mixed 2. pattern of deficit: symmetry; focal vs. diffuse; upper vs. lower limb; cranial nerve involvement 3. temporal pattern: acute vs. chronic; relapsing/remitting vs. constant vs. progressive 4. history: PMH, detailed FHx, exposures (e.g. insects, toxins, sexual, travel), systemic symptoms 5. detailed peripheral neuro exam: LMN findings, differentiate between root and peripheral nerves, cranial nerves, respiratory status |
|
|
Parkinson's genes/enviro |
Genes; - DJ-1: juvenile onset - a-synuclein - parkin Enviro: - MPTP pesticide |
|
|
Parkinson's patho |
• loss of dopaminergic neurons in pars compacta of substantia nigra=>dec dopamine instriatum=>disinhibition of the indirect pathway+dec activation of the directpathway => inc. inhibition of cortical motor areas • α-synuclein accumulates in Lewy bodies=> neurotoxicity in SN - SNc projections to putamen degenerate 1st, 2nd, projections to associative/limbic parts striatum - Corresponding tothis time course of degeneration, the motor symptoms and signs of Parkinson’sdisease develop before the non-motor signs. |
|
|
Parkinson's s/s |
- Resting tremor, pill rolling, dec w movement, reemerging - Rigidity: lead pipe/cogwheeling - Bradykinesia - Freezing gait/shuffling, postural instab - Autonomic probs: constip, urinary retention, sexual dysfunct, orthostatic hypo Behavioural/dementia (late/slowing of thinking): decreased spontaneous speech, depression, sleep probs |
|
|
Parkinson's plus features that would be suggestive |
- Early dementia - Pathologic eye mvmt - Early psychosis/ hallucinations - Severe postural instability - Symmetrical presentation - Severe autonomic dysfunction - Less/no response to Levodopa - Alien limb - recognise own limb but not the movement |
|
|
Progressive supranuclear palsy, s/s |
- Relatively symmetrical - Parkinsonism w early falls/gait disturb (first yr) - Supranuclear gaze palsy (can't voluntarily gaze down) - Insidious onset, vague fatigue, headahce, arthralgia, dizziness, depression, dysarthria, bradykinesia, visual disturbances (13%) - Clinical diagnosis |
|
|
PSP patho, epi |
- Accumulation neurofibrillary tangles in the brain |
|
|
Corticobasal ganglionic degeneration |
- Asymmetrical - Cortical (probs identifying objects, apraxia) - Basal ganglionic (usually marked rigidity in one arm) - Insidious and progressive - Depression - Dementia - Postural instab - Alien limb - Loss of ADLs |
|
|
Corticobasal ganglionic degeneration path |
Misfolded tau, frontoparietal cortical atrophy |
|
|
Multiple system atrophy |
- Symmetrical APC: - Autonomic sx - Parkinsonism - Corticospinal + cerebellar sx - Presents in 50s, F>M, die in 6-9 yrs |
|
|
MSA definition |
- Adult-onset, sporadic, rapidly progressive, multisystem, neurodegenerative fatal disease of undetermined etiology, characterized clinically by varying severity of parkinsonian features; cerebellar, autonomic, and urogenital dysfunction and corticospinal disorders. |
|
|
Distinguishing MSA from parkinson's |
MSA: • Progresses rapidly • Poor response to levodopa • Autonomic sx (urinary retention/ incontinence/ orthostatic hypotension) pronounced • Rigidity andbradykinesia>tremor • Speech isaffected severely • Aspiration,inspiratory gasps, stridor • Early falls(late in park) • No lewy bodies(at autopsy) • Badthermoregulation (cold hands) |
|
|
Lewy Body dementia |
- Parkinsonism w severe cognitive deficit w/i 1 yr - Hallucinations common (often non-visual) - Fluctuations in cognitive fcn - Daytime drowsiness - Delusions - Unexplained syncope - REM sleep disorder - Neuroleptic sensitivity |
|
|
Drug induced parkinsonism |
- Classically bilateral, symmetrical park w/o resting tremor (50% have asymm+resting trem) - 2nd most common cause of parkinsonism after PD in elderly - May persist for ages after stopping drug - Clinically indistinguishable from PD - Caused by antipsychotics, GI prokinetics, calc channel blockers, atypical antipsychotics + antiepileptics |
|
|
Signs that something is not parkinson |
Vertical gaze palsy - PSP Impotence/incontence - MSA (autonomic affected early) Visual hallucinations - DLB Intefering activity - CBD Diabetic px - vascular |
|
|
Cluster headaches mgmt |
- 02 - Tryptans - Verapamil long time
|
|
|
GBS |
- Infection trigger: campylobacter, CMV, EBV, HIC - Vaccines - Self limiting in about 4 weeks - Can die from respiratory failure - Axial>peripheral muscles - 40% you never figure - Molecular mimicry=>attacks central nerve - 1 per 100,000 per year |
|
|
Myaesthenia gravis |
- Autoimmune disorder - Problem with neuromuscular junction - 3 different problems with NMJ this is one - 15% of MG have thymic neoplasm, 85% thymic hyperplasia - s/s: (all NMJ problem) weakness, easy fatiguability, ptosis, diplopia, dysrthria, dysphagia (bulbar paresis - these four are hall mark signs). Coordination fine, movement fine - Problem is not enough acth |
|
|
Charcot Marie tooth |
- Two types - type 1: demyelination of main neurone chords with increased tissue deposition around them - Type 2: Axonal degeneration - Autosomal dominant inherited disease, myelin production, often impacts, common peroneal nerve (sural sparing), forearm, can get pain and parasthesia (can do neuronal release, peel off connective tissue) - Blindness - Diffuse deficits on EMG mgmt: good quality of life, incapacity rare - Inverted champagne bottle leg |
|
|
Cauda Equina |
- Compression/irritation lumbosacral nerve roots below conus medullaris (L2) - Aetiology: *Herniated disc +/- spinal steonisis, #vert, tumor s/s: *usually acute <24hrs *LMN signs: weakness/paraparesis in multipe root distribution. Reduced reflexes *autonomic: urinary retention, faecal incontinence, loss of anal sphincter tone *sensory: **Sciatica aggravated by valsalva/sitting relieved lying down **saddle anaesthesia **sexual dysfunction, late finding |
|
|
Abducens Palsy |
- Innervates the ipsilateral lateral rectus =>abduct ipsilateral eye. - nucleus is in pons, just ventral to the floor of the fourth ventricle and just lateral to the medial longitudinal fasciculus - Runs a long subarachnoid course - ~40% of its neurons project into the ipsilateral MLF only to cross over to the contralateral side and ascend to innervate that contralateral medial rectus subnucleus to participate in contralateral eye adduction - Binocular horizontal diplopia (double vision producing a side-by-side image with both eyes open), worse in the distance, and esotropia (both eyes look inwards) in primary gaze. - Patients also may present with a head-turn to maintain binocularity and binocular fusion and to minimize diplopia. |
|
|
Abducens palsy sign and causes |
- In soley VI nerve palsy, the only sign will be lateral gaze palsy of the ipsilateral eye - Able to adduct contralateral eye - Can be caused with inc ICP and stretching of the nerve as it ascends the clival area. - Frequently seen as a postviral syndrome in younger patients - Can be caused by ischemic mononeuropathy in adults - Can be caused by GCA |
|
|
Huntington's path |
- Autosomal dominant CAG repeats in huntington's gene on chromosome 4=>accumulation defective proteins (huntingtin) in neurones - Global cerebral atrophy, esp in striatum=>increased activity of direct pathway + decreased act indirect pathway |
|
|
Huntington's s/s |
Onset usually in 30s-40s, but can be 5-70 s/s: *Typical progression, insidious onset w clumsiness, fidfetiness, irritability=>progresses over 15 yrs to frank dementia, loss of intellectual capacity *dementia *chorea, begins w eyebrows and forehead, shrugging of shoulders, parakinesia (pseudo-purposeful mvmt to mask involuntary limb jerking) *progresses to chorea or ballism=>late stages distonia and rigidity *mood changes: irritability, depression, anhedonia, impulsivity, bouts of violence |
|
|
Guillain-Barré definition patho |
- Acute rapidly evolving demyelinating inflammatory polyneuropathy often starts in distal lower limbs and ascends - Autoimmune attack sometimes preceeded by viral/bact infections |
|
|
Guillain-Barré s/s |
- Senosory: *distal and symmetric paraesthesia *loss of proprioception *Loss of vibration sense *neuropathic pain - Motor: *weakness starting distally in legs *Areflexia - Autonomic: *blood pressure dysregulation * arrythmias *bladder dysfunction |
|
|
Myasthenia Gravis definition patho, onset |
- Progressive autoimmune d/t anti AChR abs=>early saturation NMJ=>inadequate muscle activation - 15% have thymus neoplasia - 85% have hyperplasia thymus - Bimodal onset; *20s (mostly W) *60s (mostly M) |
|
|
Myaesthenia gravis s/s |
- Occular (diplopia/ptosis) - Bulbar paresis (dysarthria/dysphagia) - Limb weakness, asymmetric, usually proximal - Resp muscle weakness may lead to resp failure - Sx may be worsened by infect, preg, menses, various drugs - No sensory, reflex or coordination changes - fatigability - Normal reflexes - Decremental response on EMG |
|
|
Corneal reflex nerves |
Afferent: Sensory Vth Efferent: motor VII |
|
|
Fourth nerve palsy eye sign |
- vertical diploplia on downwards gaze (superior oblique) |
|
|
Third nerve palsy eye signs |
- Down and out position of eye - Ptosis (III innervates levator palpebrae superioris) |
|
|
Binocular vertical diplopia |
- Prob d/t ocular misalignment (extraocular muscle issue) - Tend to close eye w dysfunctional muscle and diplopia goes away (in refractory prob will be their with binocular and monocular vision) - Usually assoc w superior + inferior recti or superior and inferior oblique lesions - Third nerve palsy often accompanied by ptosis and change in pupil size and rxns |
|
|
Diabetic ocular neuropathy most common nerve and s/s |
- Left trochlear (IVth nerve) - Complains of painful diplopia + boring pain in the orbit of the affected side - Almost always unilateral - Usually worse when reading a book or walking down stairs (looking down as IV nerve works on superior oblique) - Image can be displaced laterally and slightly tilted |
|
|
Myotonic dystrophy def |
- Most common adult MD - Autosomal dominant - Spectrum of disease based on amount of unstable CTG repeats on gene - Distal to proximal weakness in contrast to all other MDs - Life expectancy ~50 |
|
|
Myotonic dystrophy presentation |
- Ptosis - Triangular face - Bifacial weakness (dropping/dull appearance) - Frontal baldness in both men and women - Distal to proximal weakness - Steppage gait - Myotonia (delayed relaxation of muscles after contraction - ax by tapping on thenar muscs) - Cardiac ~90% have conduction problems - Hypoventilation d/t weak resp muscles - Eyes; subcapsular cataracts, inc ICP, retinal degeneration - Other: DM, infertility, testicular atrophy - No cure, manage myotonia with phenytoin |
|
|
Benign intracranial hypertension/idiopathic intracranial hypertension/pseudotumour cerebri |
- Mostly effects obese women of reproductive age - ~1 in 100,000 people - Causes papilloedema - Can progress to secondary progressive optic atrophy=>blindness |
|
|
Idiopathic intracranial hypertension s/s |
- Headaches (non-specific, varying in timing/location etc) - Diplopia and other vision changes - Pulsatile tinnitus - Radicular pain (mostly in arms, this is uncommon) |
|
|
Complex regional pain syndrome definition |
- Chronic pain condition w autonomic + inflamm features - Occurs acutely in ~7% of people w limb fractues, limb surgery or other injuries - Many cases resolve in the first year, many chronic |
|
|
Complex regional pain syndrome mechanism |
- Multiple peripheral and central mechanisms. Diff patients have different proportions of each - Include peripheral and central sensitisation, autonomic changes, sympoafferent coupling, brain changes, inflammatory and immune alterations, genetic and psychological factors |
|
|
Warm and cold complex regional pain syndromes |
- Warm: inflammatory features predominate, usually occurs in the first year - Cold: autonomic deatures predominate, transition to this usually happens ~1yr mark, this is the more common chronic version |
|
|
Complex regional pain syndrome/reflex sympathetic dystrophy s/s |
- Acute stage: 3mnths *Burning pain *Swelling and redness, vasomotor instability that worsens with dependence *Fainting *Hyperhydrosis + coolness to touch *demineralisation of underlying bone d/t disuse - Subacute stage: 9mnths *Persistent severe pain *Fixed oedema *Cyanosis or pallor, dry skin *Inc loss of fcn d/t diuse and fibrosis b/c of chronic inflamm=>fixed flexion deformity of fingers * Skin and subcut tissues atrophy *demineralisation of underlying bones pronounced - Chronic: 1yr+ *Pain may continue or abate *Odema subsides, leaving fibrosis *Skin dry, pale, cool,. shiny *Flexion and extension creases absent *Loss of fcn stiffness marked *Osteoporosis is extreme *Frozen shoulder and claw hand common |
|
|
ALS (amyotrophic lateral sclerosis) |
- Most common degenerative disease of motor neurones - Median survival 3yrs - Stephen hawking, Lou Gehrig |
|
|
ALS s/s |
- 80% px sx begin in limbs *Tripping, stumbling, awkwardness when running *foot drop *Reduced finger dexterity, cramping, stiffness, weakness *wrist drop (often interferes with work) - Bulbar onset in 20% *slurred speech, hoarseness, dec vol of speech, choking - Emotional/special cognitive: *involuntary laughing/crying *depression *impaired executive fcn *Maladaptive social behaviour Advanced disease: - Muscle atrophy - Spasticity - Muscle cramps - Voice changes, hypernasality, speech loss, drooling |
|
|
Diagnosis ALS |
- No diagnostic tools, just observation - Clinically definite ALS; UMN and LMN signs in at least 3 body segments (thoracic, lumbrosacral, cervical(arms) and bulbar (head)) |
|
|
Vertebrobasilar insufficiency definition |
- TIAs in the vertbasilar area (posterior circulation) - Usually less long lasting that carotid TIAs (average 8mins compared to 14) - Full blown stroke version of this is commonly laterally medullar syndrome |
|
|
Vertebrobasilar insufficiency s/s |
- Vertigo (hallmark sx, occurs in 33%) - Visual field defects (diplopia, hemianopia) - Auditory phenomena (sudden sensorineural hearing loss) - Facial numbness/parasthesias - Dysphagia, dysarthria, hoarseness - Syncope - Hemisensory extremity symptoms (eg. contralateral face) |
|
|
Lateral medullary syndrome (Wallenburg syndrome) |
- Lateral medulla stroke - Ipsilateral facial pain and numbness - Ipsilateral ataxia (falling to the side of the lesion) - Vertigo, nausea, vomiting - Contralateral pain and thermal impairment over body and occasionally face |
|
|
Medial medullary infarct |
- Vertebral artery stroke - Contralateral arm and leg weakness (facial sparing) - Diplopia |
|
|
Basilar artery syndrome |
- Complete basilar artery occlusion *Locked in state (awake quadriplegia) *Paralysis or weaknes of all extremities *Horizonral gaze paresis, stupor, coma |
|
|
Subclavian steal syndrome |
- Retrograde blood flow down the vertebral artery in times of increased demand of left upper limb - Stenosis of left subclavian artery causes this (just proximal to take off of vertebral artery) *Vertigo in 50% when exercising left arm (posterior circ insuff) *arm claudication and headache can also be present |
|
|
Labyrinthine artery occlusion |
- Commonly brancbhes from the anterior inferior cerebellar artery causing: *Prolonged vertigo *Hearing loss |
|
|
Acute intermittent porphyria/porphryia cutanea tarda |
- Abnormal metabolism of haem=> build up in skin, liver, CNS => aminolevulinic acid and porphobilinogen in urine Rarely acquired, but can be caused by lead poisoning |
|
|
Acute intermittent porphyria 5Ps |
- Pain in abdo - Purple urine - Psych - Polyneuropathy - Precipitated by triggers eg. drugs eg. barbituates |
|
|
Porphyria cutanea tarda |
- Etiologyuroporphyrinogen-III decarboxylase (UROD) - Susceptibility factors: *Increased hepatic iron stores *Alcohol *Hepatitis C *Sunlight exposure Clinical findings: *Cutaneous manifestations sun-exposed skin → blistering *Commonly occurs on:Dorsum of the hand |
|
|
Central cord syndrome |
- Elderly people, pre-existing spinal cord vulnerability (cervical spondylosis, syringomyelia, traumatic disc herniation) - Hits bilateral corticospinal and lateral spinothalamic tracts - Motor bilaterally upper limb>lower limb + distally>proximally |
|
|
Anterior spinal syndrome |
- Occlusion of anterior spinal artery knocks out corticospinal and spinothalamic tracts *Loss of motor, pain/temp and autonomic regulation below level of lesion (inc. bladder/rectum) - AAA surgery, trauma, burst fracture of vertebra |
|
|
Brown-sequard |
- Hemisection of the cord from trauma - Loss of ipsilateral motor + contra pain and temp |
|
|
Posterior cord syndrome |
- Trauma, occlusion of post. spinal artery, MS - Ipsilateral proprioception, vibration and touch lost below lesion (b/c dorsal tracts knocked out) |
|
|
SYRINGOMYELIA/hydromyelia |
- Formation of syrinx (fluid filled cavity) in central canal of spinal cord - Cape like distrubution of effects - Lower mtr neurones from medial cortico-spinal tract (fasiculations, areflexia, wasting)=>bilateral weakness=>bilateral flaccid paralysis + muscle atrophy over time) + loss of proprioception + vibration + horner's syndrome - 90% are congenital (chiari malformation, dandy walker), 10% acquired post SCI |
|
|
Glioblastoma multiforme |
- Adult onset brain tumour from astrocytes - Very poor prognosis - Presents usually at 65-75yrs - CT shows irregular hypodense lesion w ring-enhancing periphery (garland) involving cerebral hemispheres and possibly crossing the midline |