Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
184 Cards in this Set
- Front
- Back
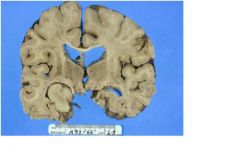
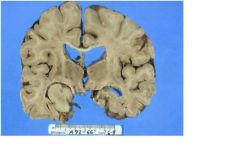
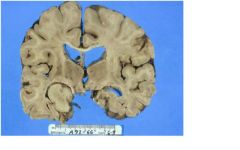
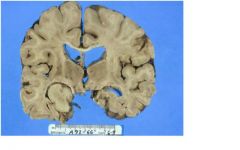
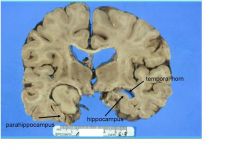
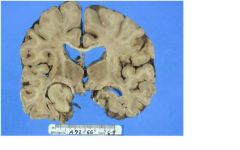
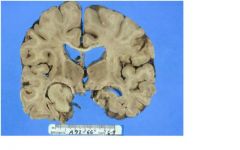
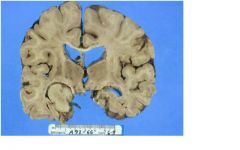
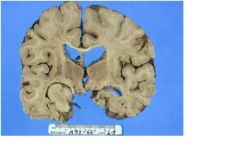
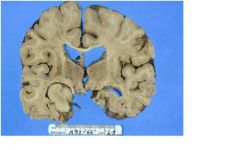
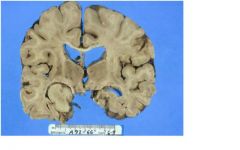
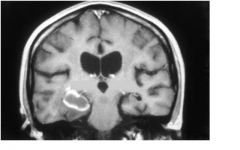
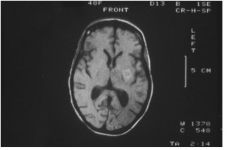
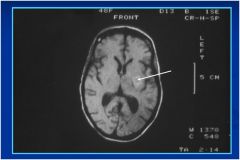
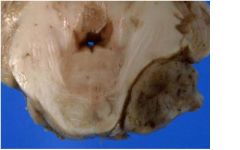
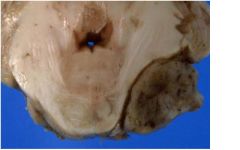
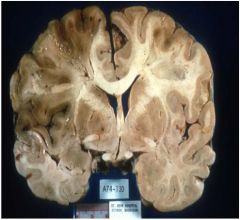
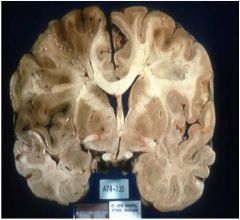
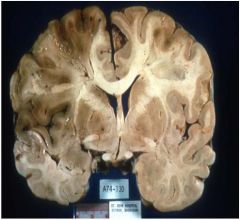
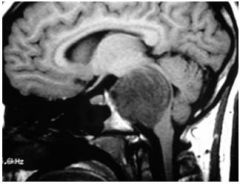
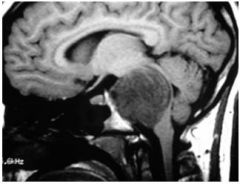
where is the lesion in this immage?
|
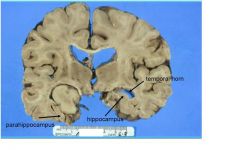
LOCATION:
MEDIAL TEMPORAL LOBE - involves hippocampus and fills temporal horn |
|
|
mass effect or local effects
|
what clinical symptoms could this person have?
|
|
|
headache
nausea/vomiting drowsiness papilledema |
What are the mass effect of this lession?
|
|
What are the local effects of this lesion?
|
seizures
disrupted HC function: ? memory - only occurs with bilateral lesions unlikely with unilateral |
|
|
fever
systemic signs |
what other sx can be seen here in this lesion besides mass or local effects?
|
|
|
What are these sx related to?
-HEADACHE (ON WAKING) -PROJECTILE VOMITING - PAPILLEDEMA - CARDIORESPIRATORY PHYSIOLOGIC CHANGES - SINUS BRADYCARDIA - IRREGULAR RESPIRATIONS - HYPERTENSION - DECLINE IN LEVEL OF CONSCIOUSNESS - NEUROGENIC PULMONARY EDEMA - FOCAL NEUROLOGIC SIGNS DUE TO TISSUE SHIFTS |
SYMPTOMS OF ELEVATED
INTRACRANIAL PRESSURE |
|
Is vision effected with this lesion?
|

Yes, you have contralateral hemienopsia
|
|
|
NEOPLASM
INFECTION HEMATOMA EDEMA |
what are possible differencial dx for this lession?
|
|
|
GLIOMA
METASTASIS |
What possible neoplasm could this lesion be?
|
|
|
CEREBRITIS
ABSCESS GRANULOMA |
what infection could result in this lesion?
|
|
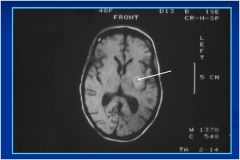
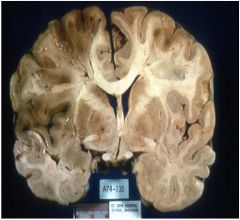
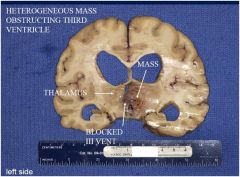
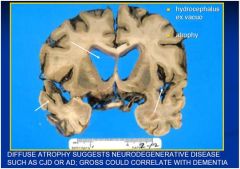
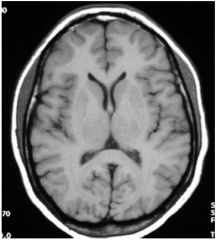
is there any problem with the ventricles?
|
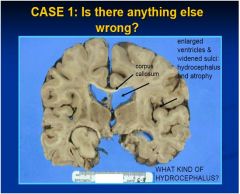
yes, hydrocephalis, review 4 types
|
|
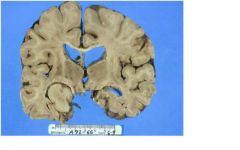
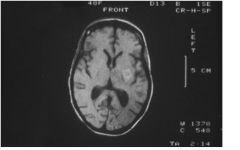
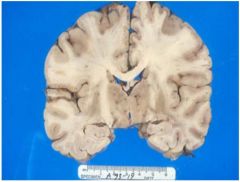
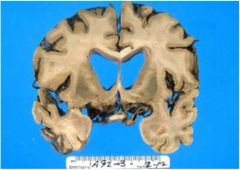
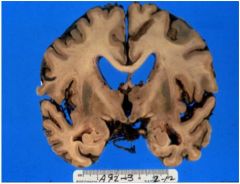
is there a problem with the sulci?
|
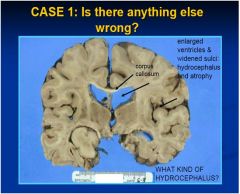
yes, the are widened meaning the brain is atrophy
|
|
|
PROBABLY HYDROCEPHALUS EX VACUO
|
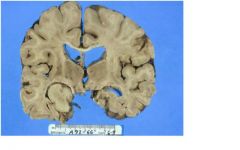
what is the dx of this pt?
|
|
|
what is the flow of csf?
|
1. LATERAL VENTRICLES
2. FORAMEN OF MONRO 3. THIRD VENTRICLE 4. CEREBRAL AQUEDUCT 5. FOURTH VENTRICLE 6. FORAMINA OF LUSCHKA & MAGENDIE |
|
|
type of hydrocephalus?
BLOCKAGE IN VENTRICULAR SYSTEM |
OBSTRUCTIVE
(NON-COMMUNICATING) |
|
|
type of hydrocephalus?
BLOCKAGE IN SUBARACHNOID SPACE, CSF-RESORPTION |
NON-OBSTRUCTIVE
(COMMUNICATING) |
|
|
type of hydrocephalus?
ATROPHY OF BRAIN |
EX VACUO
|
|
|
type of hydrocephalus?
IDIOPATHIC |
NORMAL PRESSURE
|
|
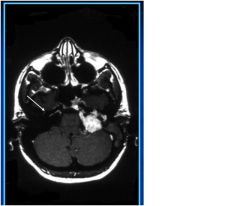
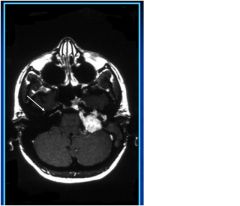
What type of study?
|

T1 MRI SCAN with contrast
-notice CSF is dark and ring enhanced mass |
|
|
cortex with acute hypoxic-ischemic damage (shrunken “red neurons”)
|
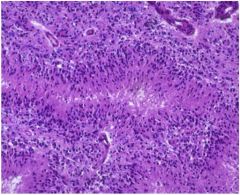
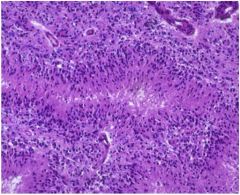
What is this?
|
|
|
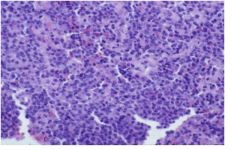
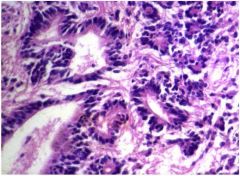
solid cellular neoplasm - lymphoma
|
what is this?
|
|
|
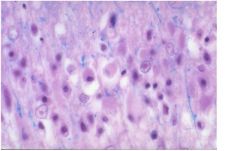
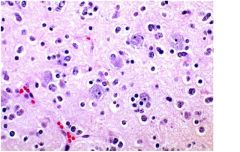
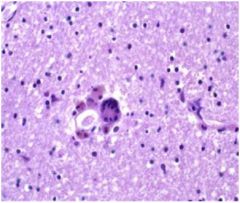
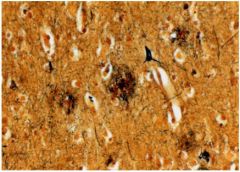
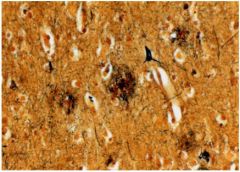
necrotic cells, intranuclear eosinophilic inclusions
(Cowdry type A): Herpes encephalitis -viral inclusion in nucleus characteristic of herpes encephalitis effecting medial temporal lobe and esp hippocampus |
what is this?
|
|
|
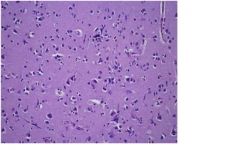
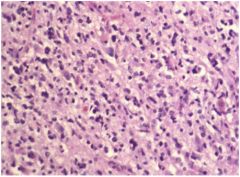
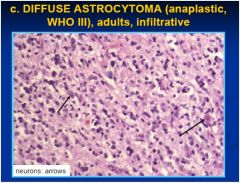
glioma: oligodendroglioma (“fried egg cells”) infiltrating cortex
-primary neoplasm in brain, does not make mass, can cause epilepsy |
what is this?
|
|

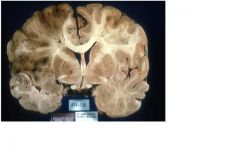
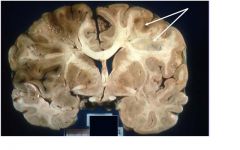
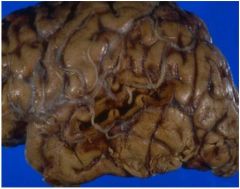
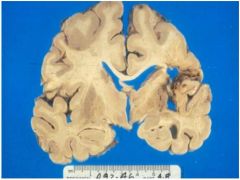
A 66-year old man with a neurologic disease who died on hospital day 5. Describe
and evaluate this picture: |

Middle cerebral artery infarct
Note mass effect + shift |
|
|
FEATURES:
left cerebral lesion: dusky, soft, well demarcated: necrotic brain |

what are the features?
|
|

What is the pathological diagnosis?
|

• encephalomalacia (brain necrosis with softening) corresponding to a particular
vascular territory • left to right shift with compression of left lateral ventricle |
|
What clinical history would fit with this picture?
|

Recent (several days) but probably sudden onset of
right-sided paresis/plegia (hemiparesis/hemiplegia) and aphasia (STROKE), now with worsening mental status due to increasing intracranial pressure |
|
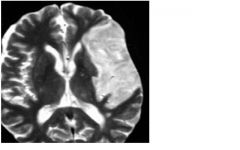
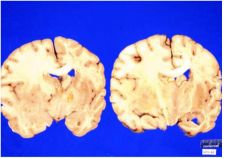
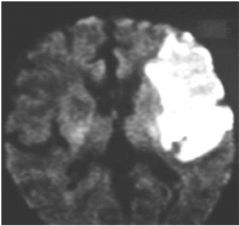
what type of image is this and what is seen here?
|
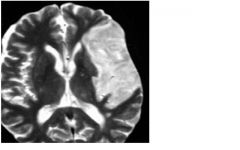
T2 MRI, CSF is bright, notice lesion on right which is edema from the necrotic area
|
|

what is unusal on the right?
|
Second infarct in watershed territory on right (btwn anterior and middle cerebral artery). Why?
Suggests a second event: embolus, hypotensive event, etc. |
|
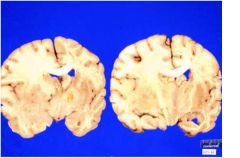
Patient with glioblastoma
multiforme diagnosed 14 months earlier: IDENTIFY: |
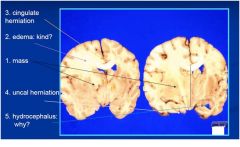
notice labeled areas
|
|
|
type of brain herniation?
herniated part: ? opening: subfalcine special effect? compression of anterior cerebral artery |
cingulate
herniated part: cingulate gyrus |
|
|
type of brain herniation?
herniated part: ? opening: tentorial incisure special effect: compression of midbrain & CNIII: coma, dilated pupil, Duret hemorrhage |
uncal (asymmetric)
herniated part: uncus (medial temporal lobe) |
|
|
type of brain herniation?
herniated part: ? opening: tentorial incisure special effect: compression of thalamus & midbrain: coma, posturing, hydrocephalus |
central (symmetric)
herniated part: diencephalon & medial temporal lobes |
|
|
type of brain herniation?
herniated part: ? opening: foramen magnum special effect: compression of medulla: apnea, acute hydrocephalus, loss of consciousness |
tonsillar
herniated part: cerebellar tonsils & medulla |
|
What kind of edema is this?
|

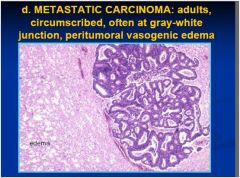
vasogenic edema secondary to tumor
mechanism: DAMAGE TO BLOOD-BRAIN BARRIER (INFLAMMATION, INFARCT, TUMOR, etc) site: WHITE MATTER |
|
|
type of cerebral edema?
DAMAGE TO BLOOD-BRAIN BARRIER (INFLAMMATION, INFARCT, TUMOR, etc) site: WHITE MATTER |
VASOGENIC
|
|
|
type of cerebral edema?
MEMBRANE ION PUMP DYSFUNCTION (HYPOXIA, TOXINS, etc) site: GRAY MATTER |
CYTOTOXIC
|
|
|
type of cerebral edema?
↑ INTRAVENTRICULAR PRESSURE (OBSTRUCTIVE HYDROCEPHALIUS) site: PERIVENTRICULAR WHITE MATTER |
INTERSTITIAL
|
|
BASED ON THE PATHOLOGY, CONSTRUCT A LIKELY SEQUENCE OF EVENTS TO EXPLAIN THE PATIENT’S DEMISE
|
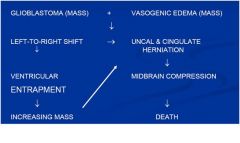
see above
|
|
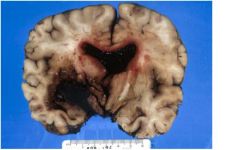
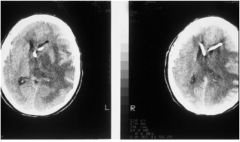
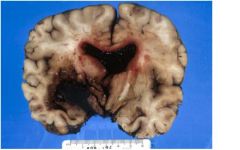
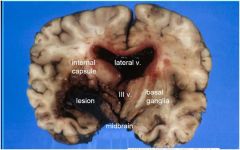
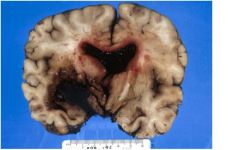
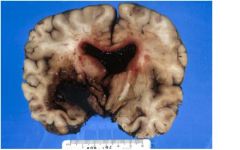
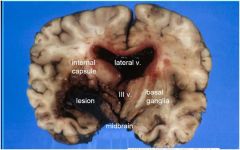
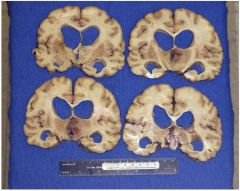
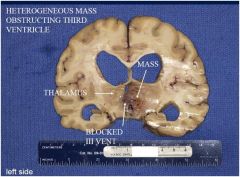
A 48-
year-old cocaine abuser with hypertension died three days after admission for persistent headache. LOCALIZE THE LESION. |
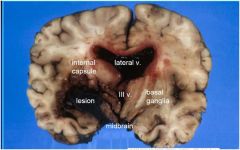
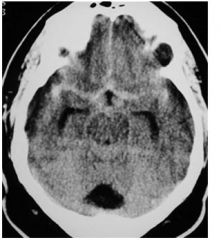
Main lesion is in left basal ganglia
|
|
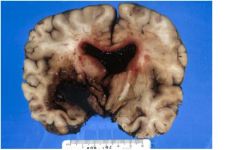
A 48- year-old cocaine abuser with hypertension died three
days after admission for persistent headache DESCRIBE THE LESION |
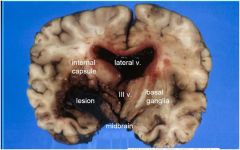
Dark red (fresh) bloody mass (hematoma)
with extension into 3rd and lateral ventricles, mass effect and L > R shift with compression of hypothalamus and midbrain |
|
A 48- year-old cocaine abuser with hypertension died three
days after admission for persistent headache PROPOSE A DIFFERENTIAL DIAGNOSIS |
Differential: acute hemorrhage due to ruptured vessel (e.g., cocaine- related), Charcot-Bouchard aneurysm from HTN, vasculitis, vascular malformation, tumor (unlikely).
|
|
A 48- year-old cocaine abuser with hypertension died three
days after admission for persistent headache PROPOSE THE LIKELY PATHOPHYSIOLOGIC SEQUENCE OF EVENTS |
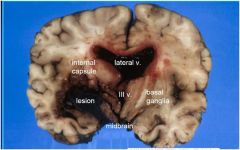
Acute cocaine-related hypertension led to rupture of muscular artery in basal ganglia; hematoma causes mass effect, dissects across internal capsule, ruptures into and fills ventricles, leading to massive increase in intracranial pressure and compression of midbrain &
hypothalamus |
|
A 48- year-old cocaine abuser with hypertension died three
days after admission for persistent headache DESCRIBE THE LIKELY SYMPTOMS/ SIGNS |
Acute excruciating headache, followed by decreased consciousness and coma,
contralateral hemiplegia, |
|
|
SUDDEN ONSET OF HEADACHE,
FOCAL DEFICITS, SIGNS OF INCREASING INTRACRANIAL PRESSURE |
INTRACEREBRAL HEMORRHAGE:
“HEMORRHAGIC STROKE” |
|
|
type of intracerebral hemmorage?
site: basal ganglia, thalamus, pons, deep cerebellum usual cause: hypertensive vascular disease outcome: fatal |
IPH: GANGLIONIC
|
|
|
type of intracerebral hemmorage?
site: cerebral lobes usual cause: various (malformation, coagulopathy. etc.) outcome: variable |
IPH: LOBAR
|
|
|
type of intracerebral hemmorage?
usual cause: berry aneurysm, AVM outcome: often lethal, acute vasospasm, chronic hydrocephalus |
SUBARACHNOID
|
|
Identify the image type and the lesion.
|
Non-enhanced T1 MRI scan - dark CSF
Degenerating subacute hemorrhage in left basal ganglia (hyperintense signal:methemoglobin). - Patient has recently bled - New massive bleed seen on gross occurred in hospital |
|
Possible etiologies?
|
Degenerating subacute hemorrhage in left
basal ganglia (hyperintense signal:methemoglobin). Possible etiologies of hemorrhage: -cocaine -hypertension (Charcot-Bouchard aneurysm - other (septic aneurysm, vascular malformation, etc.) |
|

where is the old and fresh hemmorage?
|

see above
|
|
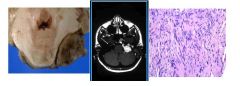
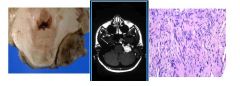
ID?
|
extra-axial solid mass indenting middle
cerebellar peduncle. Consider meningioma or schwannoma of cranial nerve VIII. |
|
type of image?
what is the arrow pointing to? |
T1 MRI with contrast
extra-axial contrast-enhancing mass, extending into internal auditory meatus (arrow) |
|
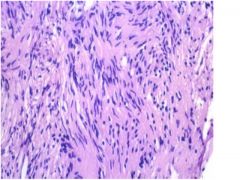
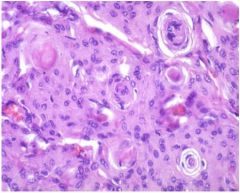
tumor type?
|
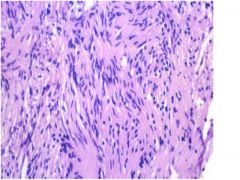
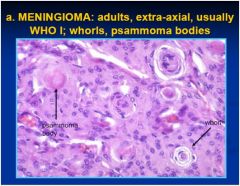
Schwannoma: note the elongate cells arranged in bundles. Tumor lacks whorls or psammoma bodies characteristic of meningioma
|
|
Construct a plausible clinical history and choose
the most likely histological diagnosis corresponding to the gross and MRI |
Adult man presenting with progressive unilateral hearing loss, possibly with
headache or mild cerebellar or vestibular symptoms. If tumor is a schwannoma, consider the possibility of neurofibromatosis type 2, especially if he has evidence of a second tumor on the opposite side or other stigmata of NF 2. |
|
|
IRREVERSIBLE LOSS OF
MULTIPLE COGNITIVE ABILITIES IN A PERSON WITH CLEAR SENSORIUM |
DEMENTIA
|
|
|
WHAT CAUSES DEMENTIA?
|
|
|
|
criteria for dementia?
|
|
|
Would this person be likely to
have had dementia? |
no bc this is an infarct which is acute and not progressive
|
|
What deficit(s) would be associated with this
lesion (only present on this side)? |

SYMPTOMS:
acute (consciousness, deficits) chronic (epilepsy, deficits) |
|
Would this person be likely to
have had dementia? |
no bc this is an infarct which is acute and not progressive
|
|
|
location of BLUNT HEAD INJURY:
CONTUSIONS AND LACERATIONS? |
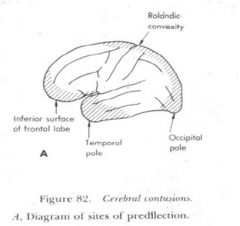
COMMON LOCATIONS: POLES, ORBITOFRONTAL, LATERAL TEMPORAL
|
|
|
irreversible, loss of cognitive functions with clear sensorium
|
dementia
|
|
|
reversible, loss of functions with clouding of sensorium
|
encephalopathy
|
|
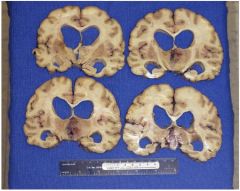
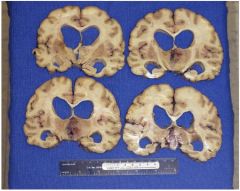
what findings can be seen here?
|
FINDINGS:
-ENLARGED VENTRICLES -NORMAL WT -ABSENCE OF CAVITIES -MASS |
|
A brain autopsy is performed on a 78- year-old cachectic man with a diagnosis of multiinfarct dementia who died after 6 months in hospice following an acute urinary tract infection
What finding is seen here? |
FINDING: NECROSIS WITH PSEUDOPALISADING
DIAGNOSIS: GLIOBLASTOMA, WHO GRADE 4 |
|
A brain autopsy is performed on a 78- year-old cachectic man with a diagnosis of multiinfarct dementia who died after 6 months in hospice following an acute urinary tract infection.
1. What other symptoms/signs should have been present? a. left hemiparesis. b. papilledema. c. cachexia. d. increased intracranial pressure. e. movement disorder. |
b, c, and d
1. What other symptoms/signs should have been present? a. left hemiparesis. b. papilledema. c. cachexia. d. increased intracranial pressure. e. movement disorder. |
|
A brain autopsy is performed on a 78- year-old cachectic man with a diagnosis of multiinfarct dementia who died after 6 months in hospice following an acute urinary tract infection
Which one of the following diagnoses best explains this patient’s history of dementia? a. Multiple old infarcts (multi-infarct dementia) led to hydrocephalus ex vacuo. b. Alzheimer disease caused hydrocephalus ex vacuo. c. Intraparenchymal hemorrhage obstructed ventricle. d. Glioblastoma multiforme obstructed ventricle. e. Chronic bacterial abscess obstructed ventricle. |
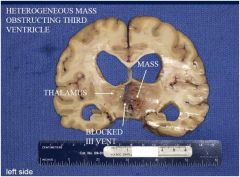
d.
Which one of the following diagnoses best explains this patient’s history of dementia? a. Multiple old infarcts (multi-infarct dementia) led to hydrocephalus ex vacuo. b. Alzheimer disease caused hydrocephalus ex vacuo. c. Intraparenchymal hemorrhage obstructed ventricle. d. Glioblastoma multiforme obstructed ventricle. e. Chronic bacterial abscess obstructed ventricle. |
|
What diesease is seen in this image?
Is it dementia? |
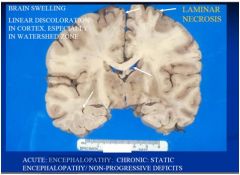
ACUTE: ENCEPHALOPATHY
CHRONIC: STATIC ENCEPHALOPATHY/ NON-PROGRESSIVE DEFICITS no demential |
|
|
What can the following cause?
-usually from profound systemic hypotension (cardiac arrest, shock, etc.) -systemic hypoxemia - hypoglycemia - CO poisoning |
DIFFUSE HYPOXIC-ISCHEMIC DAMAGE
|
|
|
what areas of the brain are damaged with:
DIFFUSE HYPOXIC-ISCHEMIC DAMAGE |
-hippocampus: Sommer's sector (CA1)
- cerebral cortex: laminar necrosis - watershed zones - cerebellum: Purkinje cells |
|
|
What condition has the following clinical conditions?
-mild damage: transient post-ischemic confusional state -intermediate damage: variable deficits, may be permanent (dementia) - severe: brain death, persistent vegetative state - “respirator brain” |
ENCEPHALOPATHY
|
|
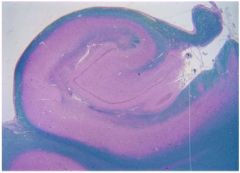
what is this structure? what area is associated with diffuse ischemic encephalopathy?
|
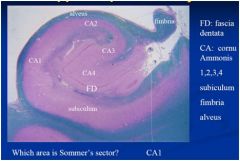
this is the hippocampus, area CA1 is refered to as Sommer sector which is one of the areas vulnerable to hypoxic ischemia
|
|
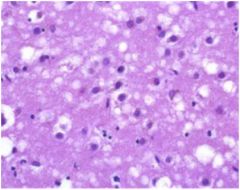
what is this?
|
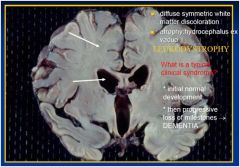
LEUKODYSTROPHIES
DEFINITION: INHERITED DISEASES WHOSE PRINCIPAL MANIFESTATIONS RESULT FROM DAMAGE TO MYELIN |
|
|
INHERITED DISEASES WHOSE
PRINCIPAL MANIFESTATIONS RESULT FROM DAMAGE TO MYELIN |
LEUKODYSTROPHIES
|
|
|
DEFECTS OF MYELIN DEGRADATIVE ENZYMES (lysosomal storage diseases)
name diseases in this category |
-METACHROMATIC LEUKODYSTROPHY
-KRABBE’S GLOBOID CELL LEUKODYSTROPHY |
|
|
disease?
DEFECTS OF MOLECULES FORMING MYELIN (dysmyelinating diseases) |
PELIZAEUS-MERZBACHER DISEASE (PLP)
|
|
what is going on here?
|
see above
|
|
What structures are involved with dementia
|

1. NUCLEUS BASALIS
2. HIPPOCAMPUS 3. MAMMILLARY BODY 4. PUTAMEN |
|
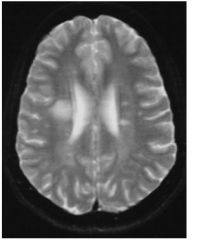
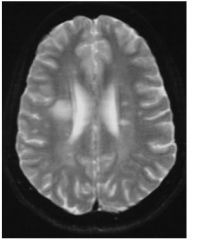
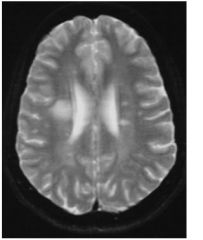
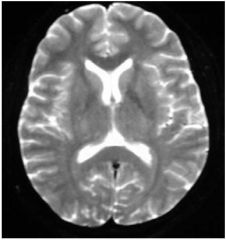
what type of image is this? What condition does this patient have?
|
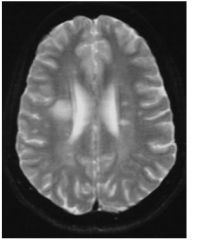
T2 MRI bc the gray matter is white and the white matter is gray.
MS |
|
What CSF findings would be seen in this pt?
|
This pt has MS. The clinical findings in the csf are:
•pleocytosis •increased protein/IgG •oligoclonal bands (electrophoresis) |
|
|
what condition has pattern of demylination in the form of plaques?
|
MS
|
|
|
what condition has pattern of diffuse perivascular demylination?
|
ADEM
|
|
|
what condition has pattern of diffuse demylination?
|
leukodystrophy
|
|
disease?
|
see above
|
|
|
common opportunistic CNS infections?
|
Toxoplasma encephalitis
PML CMV Cryptococcus meningitis |
|
|
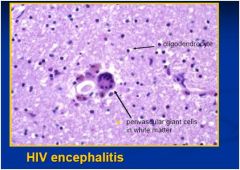
neurologic disease due to HIV infection itself
|
acute lymphocytic meningitis
chronic HIV encephalitis with progressive dementia (AIDS dementia) vacuolar myelopathy peripheral neuropathy (various types) inflammatory myopathy (polymyositis-like) |
|
disease?
|
see above
|
|
|
disease?
site: neocortex, hippocampus, n. basalis pathology: senile plaque, neurofibrillary tangles, amyloid angiopatholgy clinical presentation: dementia |
alzheimers
|
|
|
disease?
site: frontotemporal, hippocampus pathology: lobar atrophy, pick bodies clinical presentation: dementia |
Pick
|
|
|
disease?
site: substania nigra pathology: lewy bodies clinical presentation: tremor, rigidity, dec movement |
parkinson
|
|
|
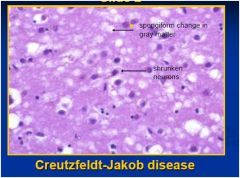
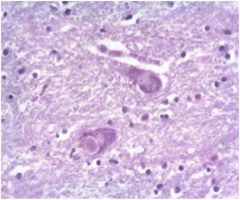
disease?
site: cortex, basal ganglia pathology: spongiform change clinical presentation: dementia, myoclonus |
CJD
|
|
|
disease?
site: caudate - putamen pathology: gaba neurons clinical presentation: chorea, dementia |
huntington
|
|
|
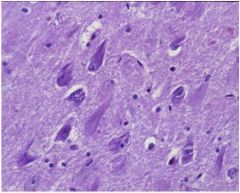
disease?
site: motor neurons pathology: UMN, LMN loss clinical presentation: paralysis, spasticity |
atrophic lateral sclerosis (ALS)
|
|
disease?
|
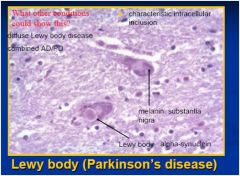
key pts: lewy bodies and the inclusions: alpha - synuclein
|
|
disease?
|
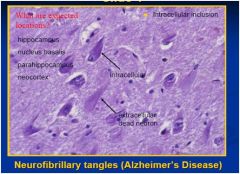
key pts: Intracellular inclusion and Neurofibrillary tangles
|
|
|
consequence of skull fracture?
|
hematoma, otorrhea, rhinorrhea, cranial nerve damage, pneumocephalus, infection
|
|
|
what do these have in common?
|
types of FOCAL BRAIN PARENCHYMAL INJURY
|
|
|
what do these have in common?
|
types of DIFFUSE BRAIN PARENCHYMAL INJURY
|
|
|
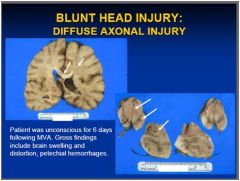
disruption/tearing of axons following sudden deceleration or torsion
|
DIFFUSE AXONAL INJURY (DAI)
|
|
|
location of DIFFUSE AXONAL INJURY (DAI)?
|
long tracts in brain stem (especially midbrain), corpus callosum, deep cerebral white
matter |
|
|
cause of DIFFUSE AXONAL INJURY (DAI)?
|
shearing/rotational forces or acceleration/
deceleration lead to tearing of axons |
|
|
symptoms of DIFFUSE AXONAL INJURY (DAI)?
|
unconscious from moment of injury
|
|

condition / disease?
|
see above
|
|
|
HEMATOMA IS ASSOCIATED WITH
SKULL FRACTURE |
EPIDURAL HEMATOMA
|
|
|
HEMATOMA IS OFTEN ASSOCIATED
WITH MILD TRAUMA IN THE SETTING OF BRAIN ATROPHY |
SUBDURAL HEMATOMA
|
|
examine the
picture and construct a plausible clinical story based on your findings and diagnosis |

see above
|
|
disease?
|
see above
|
|
cns tumor?
|
see above
|
|
disease?
|
see above
|
|
cns cancer?
|
see above
|
|
cns cancer?
|
see above
|
|
|
type of PARENCHYMAL BRAIN INJURY?
clinical feature: transient loss of conciousness (LOC) characteristic: milde DAD? |
CONCUSSION
|
|
|
type of PARENCHYMAL BRAIN INJURY?
clinical feature:loss of conciousness (LOC) +/- deficits characteristic: INTACT PIA-ARACHNOID, FRONTAL/TEMPORAL POLES, LATERAL TEMPORAL |
CONTUSION
|
|
|
type of PARENCHYMAL BRAIN INJURY?
clinical feature: loss of conciousness (LOC) +/- deficits characteristic: TORN PIA-ARACHNOID |
LACERATION
|
|
|
type of PARENCHYMAL BRAIN INJURY?
clinical feature: prolonged loss of conciousness (LOC) characteristic: TEARING OF AXONS (SPHEROIDS) IN CORPUS CALLOSUM, LONG TRACTS |
DIFFUSE AXONAL DAMAGE
|
|
|
type of TRAUMATIC VASCULAR INJURY?
source: dual arteries clinical feature: loss of conciousness (LOC), then "silent (lucid)" interval cause: skull fracture |
epidural hematoma
|
|
|
type of TRAUMATIC VASCULAR INJURY?
source: bridging veins clinical feature: acute subacute chronic cause: trauma can be mild; brain atrophy, coagulopathy |
subdural hematoma
|
|
|
type of TRAUMATIC VASCULAR INJURY?
source: parenchymal laceration clinical feature: variable cause: variable; usually severe trauma |
subarachnoid / intraparenchymal hematoma
|
|
|
type of TRAUMATIC VASCULAR INJURY?
source: shearing of axons and vessels clinical feature: similar to DAD cause: similar to DAD |
diffuse vascular injury
|
|

What is the most likely
diagnosis? a. Cord astrocytoma b. Sarcoid c. Meningioma d. Bone metastases e. Spinal hematoma |

d. Bone metastases
bc you can see lack of fat in vertebral bodies because they have been replace with tumor |
|
What type of hemorrhage is
this? a. Intraparenchymal b. Intraventricular c. Subdural d. Subarachnoid e. Epidural |

d. subarachnoid hemmorage (CT)
cistern filled with blood (bright) should be filled with dark csf |
|
|
Which imaging sequence is
the most sensitive for an acute stroke? a. T2 MRI b. CT c. T1 with contrast d. FLAIR e. DWI |
e. DWI
|
|

What space is this tumor
in? a. Intradural b. Intramedullary c. Intraaxial d. Epidural e. Intradural/Extra medullary |

d. epidural
bc out side dura, compressing sac (CT) |
|
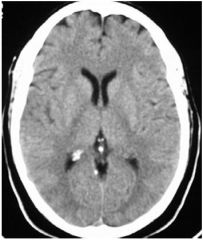
image type?
|

unenhanced ct
|
|
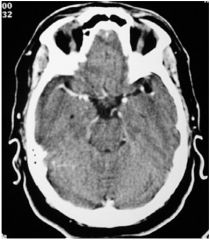
image type?
|
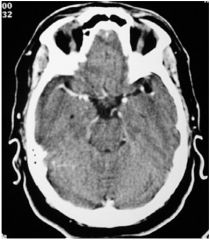
enhance ct
|
|
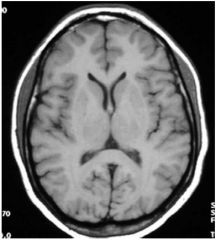
image type?
|
mri T1 axial
|
|
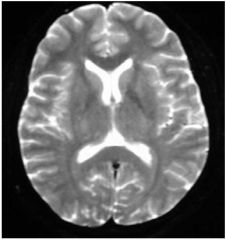
image type?
|
mri T2 axial
|
|
What Grade of Tumor is this in this patient??
|
Low grade Astrocytoma
|
|

What Grade of Tumor is this in this patient??
|

High Grade Glioblastoma
|
|
What disease would this be see in?
|
these are ALPHA-SYNUCLEIN: LEWY BODY & LEWY NEURITES
found in AD |
|
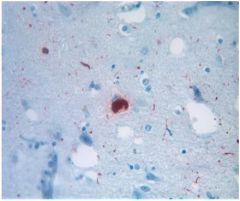
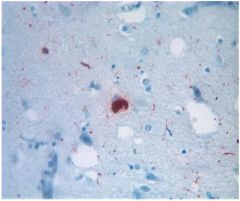
What disease does this relate to?
|
SENILE (“NEURITIC”)
PLAQUES & NEUROFIBRILLARY TANGLES (NFT) found in AD |
|
|
type of neuropathy?
-CSF shows elevated protein, usually by three days after onset of symptoms -Mononuclear cells, <10/mm3 -Pleocytosis is common with AIDP associated with HIV seroconversion -Traditionally, pleocytosis indicates polio -Electrodiagnosis shows demyelination, especially F-waves and distal latencies |
Acute, inflammatory demyelinating polyneuropathy (AIDP)
this is a category of Guillain-Barré Syndrome |
|
|
type of neuropathy?
strongly correlated with Campylobacter jejuni infection |
Acute motor axonal neuropathy (AMAN)
|
|
|
what are key points for neuropathy evaluations?
|
|
|
|
type of neuropathy?
-involves ataxia, areflexia, ophthalmoplegia (& unreactive pupils) |
Fisher syndrome
|
|
|
type of neuropathy?
-inolves antibodies against the ganglioside GQ1b, which is concentrated in oculomotor fibers and is also present on sensory ganglia. These antibodies can interfere with quantal release at neuromuscular junctions. |
Fisher syndrome
|
|
|
type of disease?
|
Presentation of Myopathy
|
|
|
type of myopathy?
• acid maltase, debrancher& brancher deficiencies • long- & very-long-chain acyl-CoA dehydrogenase (fatty acid oxidation) deficiencies • mitochondrial disease |
Metabolic Myopathies:
Progressive Weakness |
|
|
what type of myopathy do these all fit in to?
|
Toxic Myopathy
|
|
|
type of paraysis?
Sodium channel mutations |
Hyperkalemic Periodic Paralysis (HyperPP)
|
|
|
type of paraysis?
Calcium channel mutations |
Hypokalemic Periodic Paralysis (HypoPP)
|
|
|
type of paraysis?
Sodium, calcium or chloride channel mutations |
Myotonia
|
|
|
disease?
|
Myositis
|
|
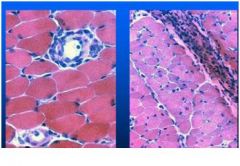
what disease type is this associated with?
|
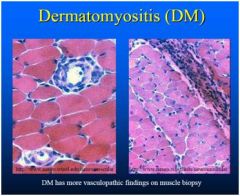
dermatomyositis - progressive weakness of muscles often with myalgia and muscle tenderness and is associated with distinctive erythematous dermatitis
|
|
|
type of dystrophy
• 1:3300 males • X-linked • Xp21 • Dystrophin Absent • CHF in late stages • 30% static encephalopathy |
Duchenne Dystrophy
|
|
|
type of dystrophy
• 1:3300 males • X-linked • Xp21 • Dystrophin reduced or abnormal • CHF in late stages • 30% static encephalopathy |
Becker's Dystrophy
|
|
|
type of dystrophy?
• 1:200,000 • Autosomal Dominant • Second decade onset • 4q35 • Scapular fixation for arm abduction • Dysphagia |
Facioscapulohumeral Dystrophy
|
|
|
type of dystrophy?
• Autosomal Dominant • Onset after age 50 • 14q11.2-q13 • Dysphagia and progressive ptosis • French-Canadian descent |
Oculopharyngeal Dystrophy
|
|
|
type of dystrophy?
• 1:8500 • Autosomal Dominant • Trinucleotide Repeat (CTG) • Myotonia • "Hatchet face" • Cardiac arrhythmias (rarely CHF) • Mild dysphagia • Cataracts and endocrine dysfunction |
Myotonic Dystrophy
|
|
|
what lab test is imp in dx of muscular dystrophy?
|
Elevated CPK
|
|
|
what disease has the following clinical features?
|
Myasthenia Gravis
|
|
|
what disease uses the following test for dx?
Tensilon test |
Myasthenia Gravis
|
|
|
what disease is treated with the following drugs?
-Pyridostigmine to enhance cholinergic transmission -Prednisone ± azathioprine -Thymectomy -Plasmapheresis |
Myasthenia Gravis
|
|
|
disease?
Caused by circulating antibodies which interfere with ACh release by binding presy |
Lambert-Eaton Myasthenic
Syndrome (LEMS) |
|
|
what disease has the following clinical features?
-Weakness and muscle fatigability similar to MG, but bulbar and respiratory muscles are less frequently involved and gait is usually affected - Autonomic dysfunction (dry mouth, sexual impotence, sometimes sphincter dysfunction) is common - Reflexes are often depressed but can be restored after a brief period of acitivty - 60% of cases are associated with small cell lung cancer |
Lambert-Eaton Myasthenic
Syndrome (LEMS) |
|
|
illusion of movement: rotation, translation or tilt
|
Vertigo
|
|
|
imbalance while standing or
walking; ataxia, proprioceptive or kinesthetic dysfunction, motor dysfunction |
Dysequilibrium
|
|
|
lightheadedness, graying out of vision
|
Presyncope
|
|
|
reset the eyes during prolonged rotation and direct gaze towards the oncoming visual scene
|
nystagmus quick phases
|
|
|
stucture in ear responsible for rotational acceleration?
|
semi-circular canals
|
|
|
fxn of vestibulo-ocular reflexes
|
gain and phase
|
|
|
holds an image of a stationary object on the fovea when the head is stationary
|
visual fixation
|
|
|
lose of vestibulo-ocular reflexes
|
oscillopsia
|
|
|
test for vestibular fxn?
• Have patient turn head 45o to one side and extend neck- this puts the posterior canal on that side in the plane of rotation • Move patient quickly from sitting to lying, letting head hang below horzontal plane- observe for nystagmus for one minute • Move patient quickly back to sitting- observe again for nystagmus for one minute • Repeat with head turned the other way to test the posterior canal on the other side |
Hallpike-Dix Maneuver
|
|
|
test for vestibular fxn?
Flush warm or cold water into one external ear canal |
Bárány’s Caloric Test
|
|
|
for the Bárány’s Caloric Test, what happens if cold water is added to one ear?
|
Cold water = nystagmus beating to the opposite side
(slow phase toward the ear being tested) |
|
|
for the Bárány’s Caloric Test, what happens if warm water is added to one ear?
|
Warm water = nystagmus beating to the same side
(slow phase away from the ear being tested) |
|
|
for the Bárány’s Caloric Test, what happens if cold water is added to both ear?
|
Cold water in both ears = nystagmus beating upward
(slow phase downward) |
|
|
for the Bárány’s Caloric Test, what happens if warm water is added to both ear?
|
Warm water in both ears = nystagmus beating downward (slow phase upward)
|
|
|
mnemonic for Bárány’s Caloric Test
|
COWS CUWD
one ear: cold water opposite nystagmus, warm water same side nystagmus both ears: cold water upward nystagmus, warm water downward nystagmus |
|
|
how is Benign paroxysmal positional vertigo (BPPV) diagnosed and treated?
|
Dx: Positive Hallpike-Dix maneuver
Rx: Epley's maneuver Modified Epley's Maneuver (prefered) • One minute to change positions, four minutes in each postion • Debris (otoconia) falls into saccule • Soft collar, no bending, sleep sitting up for two days |
|
|
dizziness for less than one minute
|
Benign paroxysmal positional vertigo (BPPV)
|
|
|
dizziness for one hour or less
|
Transient ishemic attack (TIA)
Migraine Panic Attacks |
|
|
dizziness for hours to days
|
Meniere's syndrome
|
|
|
what type of dizziness is dx and tx as follows?
Dx: fluctuating hearing loss, low frequency sensorineural hearing loss, tinnitus • Rx: Low salt diet, no caffeine, Diamox, surgery |
Meniere's syndrome
|
|
|
what type of dizziness is dx and tx as follows?
Dx: Positive Hallpike-Dix maneuver • Rx: Epley's or Semont's maneuver |
Benign paroxysmal positional vertigo (BPPV)
|
|
|
most commmon adult form of motor neuron disease
|
amyotrophic lateral sclerosis (ALS)
|
|
|
disease with gene mutation in SOD1, the gene encoding a superoxide dismutase on chr 21
|
amyotrophic lateral sclerosis (ALS)
|
|
|
disease?
without tracheostomy and ventilatory support, the life expectancy is less than 2 years after bulbar involvement. If there is predominately spinal involvement, the five year survival is approximately 20% |
amyotrophic lateral sclerosis (ALS)
|
|
|
what part of nervous system is damaged in the following NEUROGENIC MUSCLE DISEASE?
ALS, SMA, poliomyelitis |
anterior horn cell
|
|
|
what part of nervous system is damaged in the following NEUROGENIC MUSCLE DISEASE?
trauma, disc, tumor |
nerve root
|
|
|
what part of nervous system is damaged in the following NEUROGENIC MUSCLE DISEASE?
neuropathies |
peripheral nerve
|
|
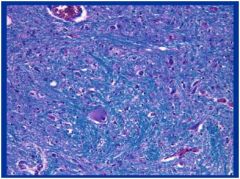
what disease is this and what clinical manifestations can be seen in this pt?
|
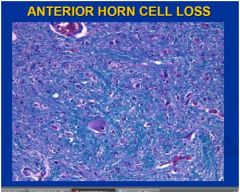
This is ALS, specifically anterior horn neuron loss associated with loss of lower motor neurons
clinical features: muscle weakness, paralysis, fasiculations, neurogenic atrophy of skeletal muscles |