![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
92 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Head Injuries Using Glasgow coma scale |
Glasgow Coma Scale |

|
|
|
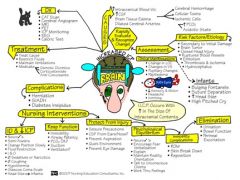
Assessment of head injuries |
4 part neuro ck
Head injury can cause--Trauma to brain tissue Intracranial hemorrhage Cerebral edema
|

|
|
|
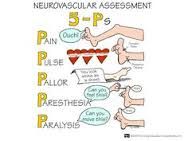
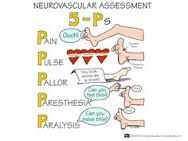
neurological assessments* |
4 parts- LOC (verbal/tactile, orientation), pupillary response (penlight outside--->in), neuromuscular response (grips/pushes), VS |
|
|
|
Prioritizing care for new head injury |
Discharge Teaching for Mild Head Injury |
|
|
|
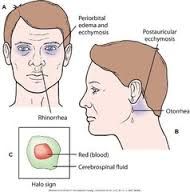
Assessing and caring for leaking cerebral spinal fluid |
halo sign
To assess CSF/ S of infec--Clear drainage from ear and nose tested for glucose with reagent strip (positive indicates CSF)
(post craniotomy)Sterile dressing over drainage, change when damp |
|
|
|
Diagnostic exams |
Head Injuries: Diagnostic Tests
Diagnostic Tests (determine cause of IICP)
CVA: Diagnostic Tests
|
|
|
|
Osmotic diuretics |
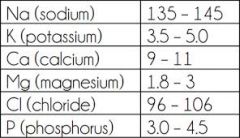
Mannitol-Closely monitor for dehydration, electrolyte losses (Na⁺ and K⁺)I & O |
|
|
|
nursing assessments and interventions |
x |
|
|
|
Nursing care of clients with head trauma, teaching |
Discharge Teaching for Mild Head Injury |
|
|
|
Basic neuro checks: how to perform and correct techniques |
4 parts- LOC (verbal/tactile, orientation), pupillary response (penlight outside--->in), neuromuscular response (grips/pushes), VS |
|
|
|
Cushing’s Triad
|
^ systolic, widening pulse pressure ie from one reading to another, goes from 98 difference to 90 difference,Bradycardia
Seen in late stage IICP |

|
|
|
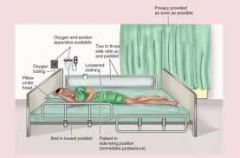
Care of unconscious client- All care including lungs skin oral bathing nutrition tube feedings etc |
W/ ICP..Assess:Breathing patterns; Babinski reflex: stroke bottom of foot (abnormal if big toe flexes upward, toes fan out); Corneal reflex: wisp of cotton to corneal surface; Gag reflex: tongue blade to back of throat; Abnormal posturing: decorticate or decerebrate; Diagnostic test results
NPO
|
|
|
|
Medications used for cerebral edema
|
Edema not tx?---> iicp
Osmotic diuretics (Mannitol) |
|
|
|
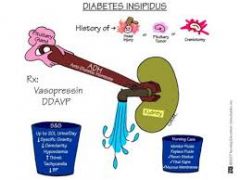
Care and assessment of diabetes insipidus |
x
|
|
|
|
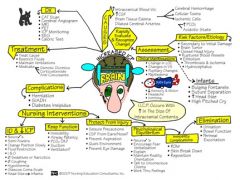
Prevention of complications that may cause IICP |
Causes of iicp--Head trauma- incl cerebral edema, brain surgery, meningitis, tumor, post craniotomy, brain abcess |
|
|
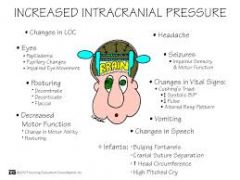
IICP: Assmt interventions s/s late/early |
Subjective:LOC, HA, N&V, Visual changes, Ringing in ears Objective Assessment: VS;Memory loss, altered thought processes;Glasgow coma scale;Pupil response: PERRLA;Grips, feet: Squeeze, push, raise legs;Drainage: ears, nose (halo sign);Raccoon eyes, Battle’s sign
Norm- 5-15mmHg
^icp leads to swelling
HOB up 30° Avoid rectal temp Breathing Nutrition Skin Mobility Infection
Osmotic diuretics (Mannitol)- For cerebral edema.Closely monitor for dehydration, electrolyte losses (Na⁺ and K⁺)I & O; Loop diuretics; Anticonvulsants (Dilantin)- Seizures; Antipyretics--Fever; Histamine antagonists or proton pump inhibitors;
Surgery to reduce IICP:
Early IICP- #1 CHANGE LOC irritable,personality changes,restless;short term memory loss; time disorientation...then place and person; perrla, decreased visual acuity, blurred vision ,diplopia; weakness to one extremety/side progessing to hemiplegia opposite brain injury site, difficulty speaking, ^bp, slightly ^pulse, RR may ^, temp may ^/decrease, HA worse on rising in a.m. and position changes
LATE- decreasing LOC..progresses to coma/no response painful stimuli, sluggish response to light progressing to fixed (no response to light). Pupils may dilate on one side progressing to bilat dialation, cannot assess vision, *decorticate/decerecrate, cannot assess speech, Cusing triad, bradycardia, decreased RR, altered resp patterns ie cheyene stokes, ^temp, continual HA, projectile vomiting, loss of -- puppil corneal, gag , swallow reflexes---Brain Herniation: |
|
|
|
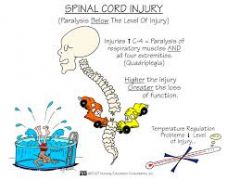
Spinal Cord Injuries Psychosocial nursing interventions |
Focus:
Situational Low Self-Esteem:
|

|
|
|
Spinal Cord Injuries Prevention of complications (all) |
Complications Life-threatening complications with cervical injury:
Spinal Shock |
|
|
|
Spinal Cord Injuries Bowel retraining |
|
|
|
|
Spinal Cord Injuries Nursing diagnoses & prioritizing |
Immediate Care
Diagnostic Tests
SCI: Stabilization and Immobilization
Halo vest Nursing care for Halo vest:
Prioritizing Nursing Care Subjective Assessment
Objective Assessment
Ineffective Breathing Pattern:
Impaired Physical Mobility:
Impaired Urinary Elimination and Constipation: Palpate bladder for fullness
Discharge Teaching:
|
|
|
|
Spinal Cord Injuries Antiinflammatory meds-- purpose s/e NX |
Corticosteroids
Antispasmodics
|
|
|
|
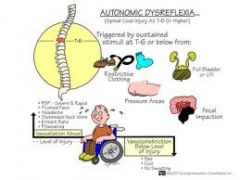
Autonomic dysreflexia-- prevention interventions meds teaching |
AD is an exaggerated sympathetic response with injury at or above T6 level.
S/S
Treatment
|
|
|
|
Herniated Intervertebral Disk-- Assessment of cervical and lumbar |
Spinal x-rays
Physical therapy Subjective Assessment
Objective Assessment
Acute Pain
Discharge teaching: |
|
|
|
Herniated Intervertebral Disk Care of client undergone laminectomy or/and diskectomy |
x |
|
|
|
Herniated Intervertebral Disk --TENS |
NSAIDs |
|
|
|
Herniated Intervertebral Disk-- Myelogram |
Nursing Care for Myelography: post procedure nursing care: |
|
|
|
Herniated Intervertebral Disk -MRI
|
x |
|
|
|
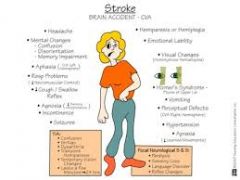
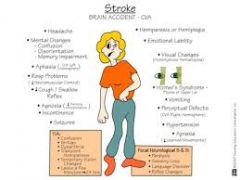
Stroke (Brain Attack/CVA)--What is it?? R/f Thrombolytic and hemorrhagic stroke- differences in care** |
Decreased blood supply to local area of brain & Leads to neurological deficits.Third leading cause of death in US, Highest incidence > 65 yrs of age,Increased risk: male, family hx of CVA, African AmericanRisk factors: CVA is sudden loss of neurologic function
Thromblytic/ischemic-- caused by artherosclerosis of large cerebral arteries, onset during or after sleep
Hemorrhagic caused by htn occuring suddenly often during some activity. Break in blood vessel aka aneurism
|
|
|
|
Stroke (Brain Attack/CVA),tx, meds, Thrombolytic therapy |
CLIENTS WITH SUSPECTED STROKE MUST RECEIVE IMMEDIATE TREATMENT (WITHIN 3 HRS) TO PRESERVE AS MUCH BRAIN FUNCTION AS POSSIBLE. Subjective Assessment: Vision, memory, confusion
Objective Assessment:
Antiplatelet to prevent CVA/clot formation--Antiplatelet Medications
Thrombolytic Medications
Anticoagulant Medications
Carotid endarterectomy
Transluminal angioplasty
Nursing care once client stable:
Activities to prevent stroke:
Public Awareness – Signs of Stroke
|

|
|
|
Stroke (Brain Attack/CVA)Emotional imbalances with stroke |
Cognitive and behavior changes:
|
|
|
|
Stroke (Brain Attack/CVA) Communication**/eye sight/sensory problems |
Speech Deficits
Impaired Verbal Communication
Visual deficits
Sensory-perceptual deficits: Disturbed Sensory Perception
|
|
|
|
Stroke (Brain Attack/CVA) Contralateral effects |
Strokes usually occur in one hemisphere
Motor deficits: (weakness, paralysis, or spasticity) Motor deficits: |
|
|
Heparin/Coumadin/labs |
note--Anticoagulant Medications |
|
|
|
Oral care/skin care |
Immobility complications:
CVA-Impaired Urinary Elimination and Constipation |
|
|
|
catheter insertion and care
|
CVA GU problems-Incontinence, frequency, urinary retention |
|
|
|
respiratory care |
Cva Respiratory problems |
|
|
|
prevention of immobility complications |
CVA probs
CVA-Self-care deficits
Immobility complications: |
|
|
|
feedings with dysphagia/tube feedings |
GI problems CVA--Impaired Swallowing |
|
|
|
Monitoring urinary output
|
x |
|
|
|
Transfer techniques
|
x
|
|
|
|
Lung/heart assessment and complications |
x
|
|
|
|
Giving Lasix
|
x |
|
|
|
DNR clients following stroke/nursing responsibilities
|
x
|
|
|
|
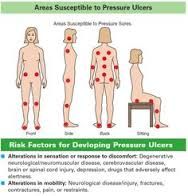
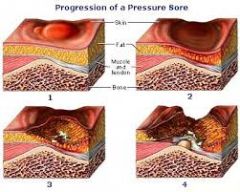
Care of pressure ulcers |
x |
|
|
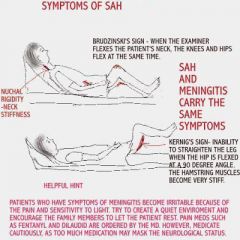
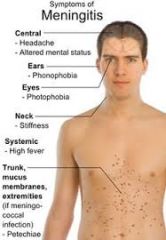
Neuro Disorders- Meningococcal meningitis/viral |
Bacterial Meningitis Inflammatory response begins
HA, high fever
Meningitis Complications:
Meningococcemia
Bacterial Meningitis
Bacterial Infections |
|
|
|
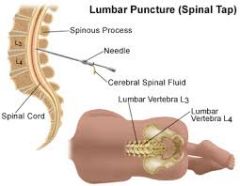
Neuro Disorders- Lumbar puncture |

Preprocedure:
Post Procedure: |
|
|
|
Neuro Disorders- Migraines |
common, unknown cause- r/f woman, fam hx, Triggers- stress/crisis/foods ie alcohol, chocolate, caffeine, nuts,monthly cycle hrs--days duration If w/ aura-- usually <1h
Nx: identify cause-- brain scan MRI xray of skull cervical spine EEG lumbar puncturefor csf, if systemic probs suspected- serum metabolic screen/ hypersensitivity testing
Subjective Assessment:
Objective Assessment
meds -Amitryptoline
Acute Pain
Clients with long-term or migraine headaches
|
|
|
|
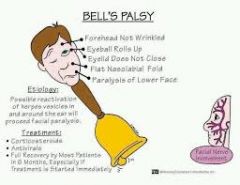
Neuro Disorders-Bell’s Palsy
|
Bell’s palsy – facial paralysis
Symptoms
Medications:
Teach:
|
|
|
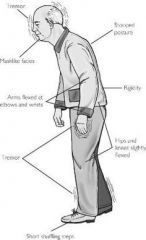
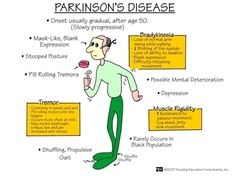
Neuro Disorders- Parkinson’s Disease |
Most common neurologic disorder in the U.S.
Deficiency of dopamine
Onset gradual
Goal:
No specific tests to diagnose PD Four drug classes:
Dopaminergics
Dopamine Agonists
Surgery Electrical Stimulation Subjective data assessment:
Objective data assessment:
Impaired physical mobility
Impaired verbal communication
Imbalanced nutrition; less than body requirements
Discharge teaching:
|
|
|

Neuro Disorders-Multiple Sclerosis |
Caucasian females
Cause:
Onset
Autoimmune response triggered by virus
Periods of exacerbation and remission
Disease progresses:
Goal:
Diagnosis
Medications
Physical therapy Plasmapheresis
Well-balanced diet Assess:
Fatigue
Self-Care Deficits Discharge teaching:
|

|
|
|
Neuro Disorders-Myastenia gravis |
Chronic, autoimmune disease
Unknown cause
Eyelid ptosis
Two possible life-threatening emergencies:
Diagnosis
Anticholinesterase Medications Anticholinesterase Medications: Anticholinesterase medications administered on strict time schedule: Assessment:
Discharge teaching:
|
|
|
|
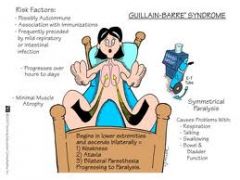
Neuro Disorders-Guillain Barre’ Syndrome |
Acute, progressive inflammation of peripheral nervous system (PNS)
Immune response destroys myelin sheath covering peripheral nerves
Symptoms start in lower extremities and move upward
Diagnosis
Most clients recover
Plasmapheresis
Managed in ICU |
|
|
|
Neuro Disorders-Huntington’s Disease |
Inherited neurologic disease
Intellectual function
No specific test
Meds given to control symptoms
|

|
|
|
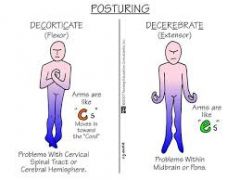
Posturing |
x |
|
|
|
decerbrate vs decorticate |
either of these seen late stages iicp |
|
|

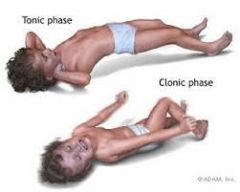
Tonic-clonic seizures |
Tonic-Clonic Seizure (Grand Mal):
Aura Phase
Status Epilepticus--Continuous tonic-clonic seizure Status Epilepticus Treatment:
http://www.youtube.com/watch?v=4CNmWpowFTM
Electroencephalography (EEG)
|
|
|

Post-ictal phase of seizures |
Unconscious for up to 30 min |

|
|
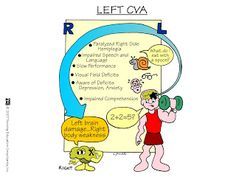
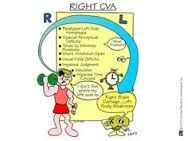
CVA-- L vs R |
|

|
|
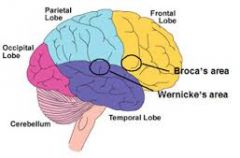
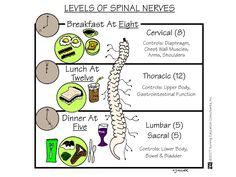
Neuro anatomy |
|
|
|
|
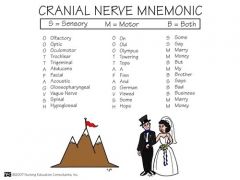
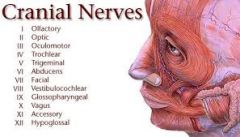
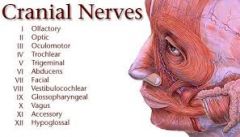
Cranial nerves
|
|
|
|
|
Efferent vs afferent neurons in regards to CNS |
Senory (afferent) neurons – carry impulses from skin and muscles to CNS |
|
|
|
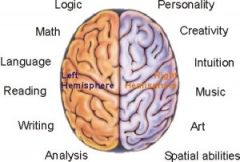
R & L hemispheres-- Where do sensory/motor impulses come from? What do both the R and L hemisphere control? |
Each hemisphere receives sensory and motor impulses from opposite side of body |
|
|
|
The brain-- diencephalon |
Diencephalon includes:
|
|
|
|
3 componenets of brain stem and what they control |
Brainstem
|
|
|
|
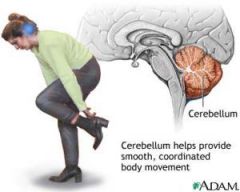
Cerebellum |
Connected to brainstem |
|
|
|
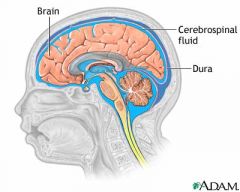
CSF |
Four ventricles in brain make CSF |
|
|
|
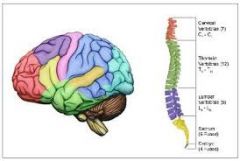
Spinal chord- gray vs white matter
|
Inside of spinal cord is H shaped, consists of gray matter surrounded by white matter |
|
|
|
Somatic vs autonomic system of PNS |
Somatic nervous system – connects skin and muscles to CNS |
|
|
|
Cranial nerves-- 12 pairs |

|
|
|
|
fx autonomic system (ANS)* |
Maintains homeostasis
|
|
|
|
ANS-- Sympathetic nervous system (SNS) |
Prepares body to handle stress |

|
|
|
ANS- Parasympathetic Nervous System (PNS) |
•Operates during nonstressful situations |
|
|
|
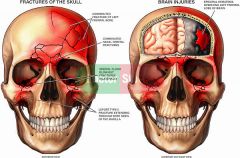
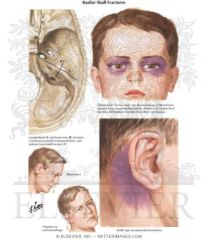
4 types of skull fractures* |
Linear
|
|
|
|
Open vs closed head injury |
Open Head Injury |
|
|
|
Linear fracture head |
simple clean break |
|
|
|
Comminuted head fracture |
shatters into peices |
|
|
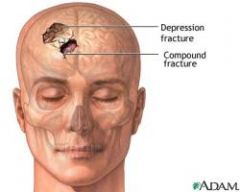
Depressed head fracture |
skull bone fragments pushed into brain |
|
|
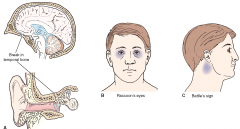
Basilar head fracture |
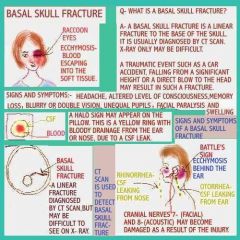
Basilar skull fracture may extend to nasal sinus or middle ear
|
|
|
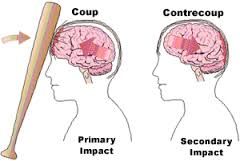
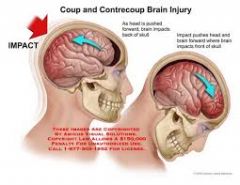
Coup-Contrecoup |
•Brain bounces forward (acceleration) and rapidly rebounds (deceleration) and hits the back of the skull |
|
|
|
concussion vs contusion |
Concussion--Brain injury caused by violent shaking of brain Post Concussion Syndrome
Contusion is Bruising of brain tissue when brain strikes inner skull
|
|
|
|
Brain tumor- s/s , diag, tx, nx |
General S/S:
CT scan
Chemotherapy
Brain Tumor: Nursing Care |
|
|
|
Craniotomy |
Preop Care:
Postop Care: Prevent infection Assess for CSF leak from ears, nose, or wound
Discharge Teaching:
Client to Report:
|

|
|
|
TIA |
Brief episode of reversible neurologic deficits
Signs of TIA: |
|
|
|
Nx CT scan head |
Nursing care for CT scan
|
|
|
|
CVA surgery- NX carotid endarterectomy |
Prevent stroke Nursing Care Post Carotid Endarterectomy
|
|
|
|
Cerebral Aneurysm: Symptoms |
•Expanding aneurysm:
complications--Ruptured aneurysm - major complications:
CT scan
Cerebral Aneurysm: Medications
Surgery
Care if surgery prohibited
|
|
|
|
Seizures- Causes, patho, types, meds, nx, surgery, prioritization |
Seizure - abnormal electrical activity in brain
Causes for seizures:
Seizure activity greatly increases metabolism
Absence seizure (Petit mal)
Tonic-Clonic Seizure (Grand Mal):
Anticonvulsant medication Klonopin (clonazepam) Nursing Implications:
Surgery
Goal:
|

|
|
|
Seizures: Electroencephalography (EEG) nursing care: |
•Explain procedure |
|
|
|
Seizures- , assmt ,Nx, prioritization, teaching |

Goal:
Subjective assessment
Objective assessment
Risk for ineffective airway clearance
Risk for injury
Anxiety
Discharge Teaching:
|
|
|
|
Encephallitis |
Inflammation of white and gray matter S/S similar to meningitis: |
|
|
|
Brain Abscess |
•Purulent matter in brain |
|
|
|
Intracranial Infections: Diagnostic Tests, meds, nx |
•Lumbar puncture
Bacterial Infections
Risk for ineffective cerebral tissue perfusion
Acute pain
|
|