Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
What are some examples of dysfunctions of the cerebral cortex? |
- Seizures
- Metabolic derangements - Toxins (alcohol, hallucinogens, sedatives, liver/kidney dysfunction) - Stroke - Migraine - Psychiatric disorders - Trauma - Tumor - Neurodegeneration - Infection |
|
|
What are the levels of consciousness?
|
- Awake state
- Sleepy - Stupor - Coma |
|
|
What level of consciousness is characterized by being able to maintain alertness, attention, awareness including awareness of self and environment?
|
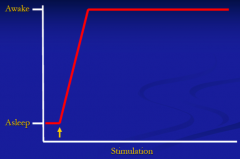
Awake state
|
|
|
What level of consciousness is characterized by waning alertness after short periods without stimulation?
|
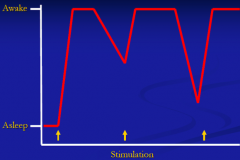
Sleepy
|
|
|
What level of consciousness is characterized by severely impaired alertness; attention, awareness only maintained with continued stimulation?
|
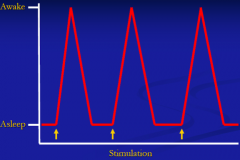
Stupor
|
|
|
What level of consciousness is characterized by loss of alertness, attention, awareness and arousability?
|
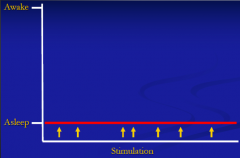
Coma
|
|
|
What state is characterized by being alert and aware but attention severely impaired / confused?
|
Delirium
|
|
|
What state is characterized by all 3 domains affected (alertness, attention, and awareness), but to a lesser degree than in a coma (some alertness maintained)?
|
Encephalopathy
|
|
|
What is similar about most patients with altered consciousness (from delirium to coma)?
|
Either structural or functional abnormalities in one of the following regions:
- Diffuse bilateral cerebral hemispheres - Bilateral thalami - Brainstem ARAS (ascending reticular activation system) |
|
|
Why is there altered consciousness in "diffuse bilateral cerebral hemispheres"?
|
- Because both hemispheres involved
- If only half the cerebrum involved, typically will NOT have altered consciousness (although they will have focal deficits) - MRI: anoxic brain injury bilaterally to cortex and thalami |
|
|
Why is there altered consciousness in "bilateral thalamic lesions"?
|
Because ARAS (ascending reticular activation system in brainstem) projects here on the way to the cerebrum
|
|
|
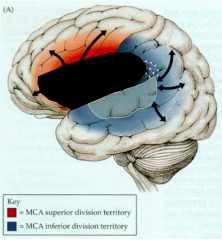
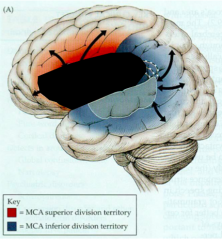
What arteries supply the frontal lobe with blood?
|

- Middle Cerebral Artery
- Anterior Cerebral Artery |
|
|
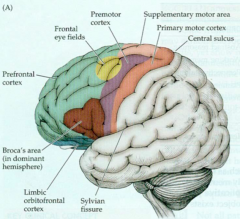
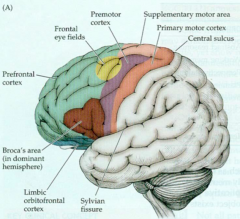
What are the important cortical areas of the Frontal Lobe?
|
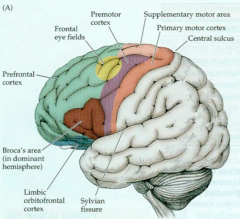
- Primary Motor Cortex
- Frontal Eye Fields (FEF) - Broca's Area - Prefrontal Cortex - Orbitofrontal Cortex - Mesiofrontal Cortex |
|
Primary Motor Cortex
- Functions? - Symptoms if lesioned? - Symptoms if activated (seizure)? |

- Voluntarily controls contralateral movement
- Lesion: contralateral hemiparesis - Activation: contralateral clonic movements; Jacksonian March (seizures travel along gyrus and activate muscles in order seen on motor homunculus) |
|
Frontal Eye Fields (FEF)
- Functions? - Lesions? |
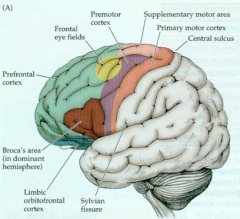
- Contralateral saccades - voluntary eye movements to contralateral field (R FEF --> look L)
- Lesion: Ipsilateral gaze preference (think tongue - CN XII) - E.g., L FEF stroke --> L gaze preference |
|

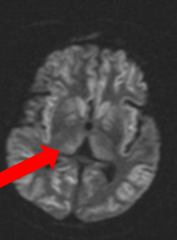
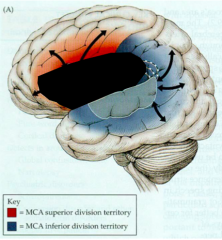
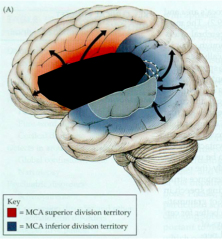
What explains this patient's symptoms?
|

- Hemiparesis on R side --> L primary motor cortex
- Eye movements to L side --> L frontal eye fields (FEFs) - Both supplied by L MCA |
|
|
Broca's Area
- Functions? - Location? - Loss of function? |
- Fluency of language
- Inferior frontal lobe in dominant hemisphere (for most it is L, but for some L handers it is bilateral) -- supplied by MCA - Loss of function: Broca's Aphasia - Non-fluent Aphasia (non-fluent, halting, effortful speech, composed of only a few words that make sense) |
|
What are the characteristics of a Broca's Aphasia?
|
- Non-fluent Aphasia
- Speech is non-fluent, halting, effortful, composed of only a few words that usually make sense - Comprehension intact - Agrammatic - Repetition impaired |
|
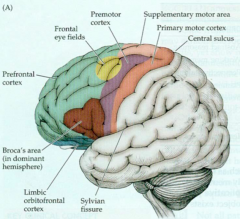
Prefrontal Cortex
- Functions? |
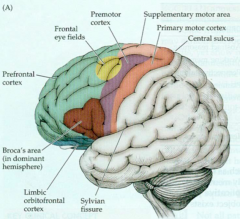
- Provides ORDER
- Mediates personality, executive function, ability to sequence and organize tasks, abstract / problem solving |
|
|
Orbitofrontal Cortex
- Functions? - Location? - Injury? |
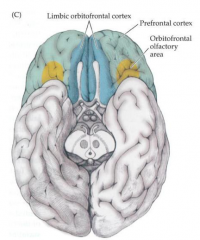
- Provides RESTRAINT
- Inhibits socially inappropriate behavior - Part of limbic system (plays role in memory and emotions) - 2 most common ways to lesion: head trauma as it rubs along base of skull or meningioma (tumor of meninges at base of skull) |
|
|
What parts of the brain are injured during head trauma?
|

- Anterior tips of temporal poles
- Orbitofrontal cortex - Occipital poles |
|
|
If a patient has a drastic change in personality, what part of the brain is responsible?
|
Prefrontal cortex (responsible for order)
|
|
|
If a patient has poor judgment (change from usual), what part of the brain is responsible?
|
Prefrontal cortex (responsible for order)
|
|
|
If a patient has inappropriate behaviors (sex with strangers) (change from usual), what part of the brain is responsible?
|
Orbitofrontal Cortex (responsible for restraint)
|
|
|
Case: Symptoms began 12 y ago, when patient became easily irritable, began drinking excessively, had sexual intercourse with homeless men, and became increasingly quarrelsome. After 6-8 years she could no longer hold down a job, neglected her hygiene, and started having crazier behaviors.
What is her diagnosis? Why? |
Frontotemporal Dementia (Pick's Disease)
- Changes in personality --> prefrontal cortex - Poor judgment --> prefrontal cortex - Inappropriate behavior --> orbitofrontal cortex |
|
|
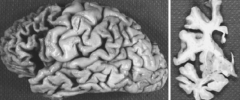
What are the characteristics of Frontotemporal Dementia (Pick's Disease)?
|
- Progressive dementia due to neurodegeneration
- Affects prefrontal cortex first --> personality changes, irritability, mood changes, poor executive function - Eventually affects other regions of frontal cortex such as orbitofrontal cortex and temporal cortex - Dementia occurs in mid life (50s) - much earlier than most cases of Alzheimer's - Shortened lifespan |
|
|
Mesiofrontal Cortex
- Functions? - Lesion? |
- Provides INITIATIVE
- Motivation and goal-directed behavior - Micturition Inhibitory Center - Lesion: akinetic mutism (no moving/talking), abulia (lack of initiative), and incontinence as seen in hydrocephalus (ventricles enlarge and stretch fibers traveling medially to spinal cord) |
|
|
What are the cortical areas in the Parietal Cortex?
|
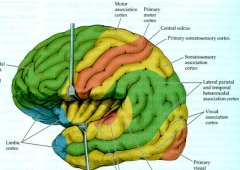
- Primary Somatosensory Cortex
- Association Cortex - Non-dominant Association Cortex (R) |
|
|
Primary Somatosensory Cortex:
- Functions? |
Contralateral sensation
|
|
|
Dominant Parietal Somatosensory Association Cortices:
- Functions? |
- Mediates higher order sensation
- Graphesthesia (ability to discern what is written on skin) - Stereognosis (ability to discern object placed in hand) |
|
|
Non-dominant Parietal Somatosensory Association Cortices:
- Functions? - Lesion? - Location? |
- Drives spatial attention on both hemifields (R parietal cortex controls spatial attention on L hemifield >> R hemifield; L parietal cortex controls spatial attn on R hemifield primarily)
** Drives attention to world ** - Lesion: contralateral neglect and apraxia - Usually on R side |
|
|
What is Graphesthesia? What part of the brain mediates it?
|
- Ability to discern what is written on hand
- Parietal somatosensory association cortices |
|
|
What is Stereognosis? What part of the brain mediates it?
|
- Ability to discern an object placed in the hand based on sensation
- Parietal somatosensory association cortices |
|
|
What is Neglect? What part of the brain mediates it?
|
- Not paying attention to contralateral hemifield
- Right side (nondominant association cortice in parietal lobe) is most important for driving attnetion to the world - E.g., R parietal lesion --> severe L neglect, ignore L side of world, bump into objects on L side, ignore L side of body |
|
|
How can you assess Neglect?
|
- Have a patient bisect a line in the middle (neglect = off-center)
- Have them bisect all the lines on a piece of paper in the middle (neglect = only bisect on one half) - Have them circle a certain letter on a page full of letters (only circle letter on one half) |
|
|
When you have a patient draw the face of a clock, put all the numbers in, and put the hands at 10 past 11, what are you assessing?
|
- Neglect (non-dominant association cortex of parietal lobe)
- Executive function (prefrontal cortex) |
|
|
What is Apraxia?
|
- Inability to perform a skilled task (e.g., brushing teeth, combing hair, dressing, tying shoe lace)
- Ability to execute a learned task = PRAXIS |
|
|
What is Gerstmann Syndrome?
|
- Lesion of dominant (L) parietal cortex (angular gyrus)
- 4 components to clinical syndrome: - Agraphia (inability to write) - Acalculia (inability to calculate) - Finger Agnosia (inability to recognize fingers) - R/L confusion (can't discern between R and L) |
|
|
What are the cortical areas of the Temporal Lobe?
|
- Wernicke's Area
- Medial Temporal Lobe |
|
|
Wernicke's Area
- Functions? - Location? - Lesion? |
- Comprehension of language
- Superior temporal gyrus in dominant hemisphere (usually L) - Lesion: fluent aphasia - lots of nonsensical gibberish (may or may not be aware that it is not correct despite not comprehending); can't follow commands, impaired repetition - Small branch of MCA |
|
|
What are the characteristics of Conduction Aphasia? What can cause it?
|
- Inability to repeat
- Arcuate fibers damaged - Smaller branch of MCA stroke |
|
|
What are the characteristics of Global Aphasia? What artery can cause a stroke in this area?
|
- Impaired comprehension, repetition, and fluency
- Usually no language - Due to full MCA stroke at its proximal origin (where ICA divides into ACA and MCA) |
|
|
What are the symptoms of Kluver-Bucy Syndrome?
|
- Hyperorality (pt explores environment w/ mouth)
- Inappropriate sexual displays (removing clothes, masturbation in public, inappropriate kissing/flirting) - Irritability and aggression - Anterograde amnesia (amygdala) - Alternating episodes of depression and overactivity |
|
|
What causes Kluver-Bucy Syndrome?
|
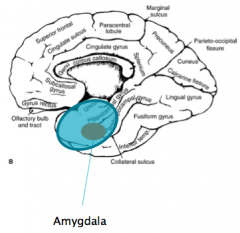
Bilateral anterior temporal poles and bilateral amygdala injuries (commonly from head trauma)
|
|
|
What issues affect the medial temporal lobe?
|
- Hippocampal atrophy - neuronal degeneration in hippocampus occurs early in Alzheimer's disease
- Hippocampal sclerosis - scarring of hippocampus is thought to cause or be the result of uncontrolled complex partial seizures |
|
|
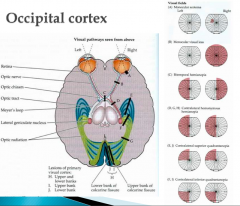
What are the areas of the cortex in the Occipital Lobe?
|
Primary Visual Cortex
|
|
|
What problems are associated with defects in the primary visual cortex of the occipital lobe?
|
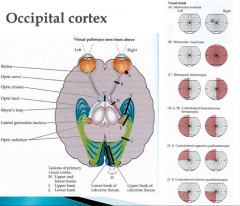
- Visual field defects (VFD)
- Monocular VFD --> lesion anterior to chiasm - Binocular VFD --> lesion posterior to chiasm - Homonymous = affecting both sides |
|
|
If there is a lesion to the RIGHT occipital cortex, how will vision be affected?
|
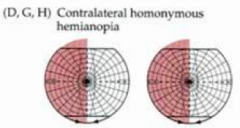
- L Homonymous Hemianopia
- Right occipital cortex mediates vision from Left hemifield of both eyes |
|
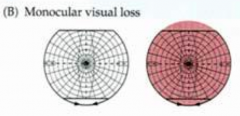
If there is a monocular visual defect, what is likely the cause?
|
Lesion anterior to the optic chiasm (B)
|
|
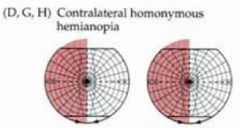
What does a homonymous hemianopia tell you about the lesion?
|
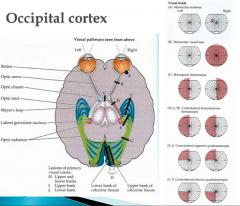
- Affects both sides
- E.g., R homonymous hemianopia indicates that R field on both eyes are affected - Indicates a lesion in the cortex / subcortex |
|
|
What structure connects the lateral geniculate nucleus and the visual cortex?
|
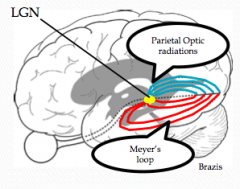
Optic Radiations
|
|
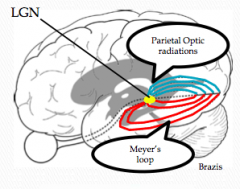
How does a lesion to the optic radiations affect vision?
|

- Lesion to Meyer's loop (temporal optic radiations) --> contralateral superior quadrantanopia
- Lesion to Parietal Optic Radiations --> contralateral inferior quadrantanopia |
|
|
How does a PCA stroke affect vision?
|
- Homonymous hemianopia with macular sparing
- May occur due to dual blood supply to occipital pole (PCA and MCA) - Outer tip of calcarine cortex is representative of macular vision - Inner portions of calcarine cortex represent peripheral vision |
|
|
What are the symptoms of Balint Syndrome?
|
- Simultanagnosia (inability to perceive visual field as a whole)
- Optic Ataxia (inability to point to objects in visual field) - Ocular Apraxia (inability to look at objects in visual field using saccades) |