Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
41 Cards in this Set
- Front
- Back
|
What is the bacteriology of Mycobacterium?
|

Mycobacterium: Slim, weakly Gram (+) bacilli, acid-fast (red), req/ heat to stain through cell wall lipids, non-motile, strict aerobes, classically cause chronic granulomas (high infectivity but low virulence)
------------------------------- Mycobacterium tuberculosis in sputum stained by the acid-fast technique. The mycobacteria retain the red carbol fuchsin through the decolorization step. The cells, background, and any other organisms stain with the contrasting methylene blue counterstain |
|
|
What composes the Mycobacterium cell wall?
|
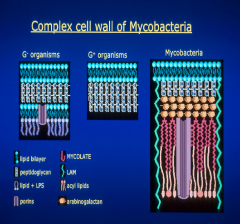
60% is lipid making it very hydrophobic & resistant to drying & resistant to chemical agents. It is a heterogeneous bilayer.
Majority of this is Mycolic acid which causes it to gram stain poorly but once it is retained it is acid fast in resisting washing out the stain |
|
|
How do you get a 1y TB infection?
|
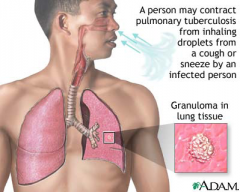
Typically from Aerosol from active TB cases. UV kills microbe, so prolonged exposure in dark enviroment harbors spread. This will then deposit in lung, be ingested by macrophage leading to granuloma formation If exposed 10-30% become infected.
|
|
|
What is the 1y pneumonia pathogenesis?
|

Mycobacterium tuberculosis deposits in lower lobe -> TB is ingested by alveolar macrophage -> TB mycolic wall permits intracellular proliferation/survival. -> infection spreads hilar lymph, blood -> Spread stops once DTH/CMI forms tubercule that is walled off.
|
|
|
What does reactivation or latent tuberculosis look like?
|
The same as a 1y infection. This was caused by reactivated TB. Notice the fibrosis that surrounds the tubercle. Their is likely more fibrosis in latent.
This ability to decrease metabolism is a virulence factor to allowing it to persist. |
|
|
How is 1y TB infection different from latent infection?
|
A weakened T cell response or immunocompromised state leads to reactivation from the dormant state. No initial inoculation from another infected individual is required.
|
|
|
What is the pathogenesis of reactivation or latent tuberculosis?
|
A decreases in T cell response(AIDs, age, stress) -> reactivation of apex located tubercles -> TB replication results in cavitation -> TB, necrotic debris, blood are released to bronchi -> active TB that is highly contagious
10% TB will reactivate. TB may spread to bone or CSF |
|
|
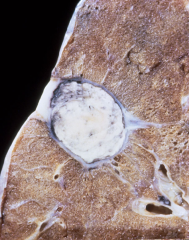
What is the classical appearance of 1y tuberculosis on Xray?
|
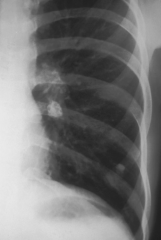
Ghon complex - benign healed 1y TB lesion. Calcified hilar lymph node (upper and medial) & granuloma (lower and lateral)
Calcification is after recovery from infection (where located in this image) |
|
|
What does the Tuberculin PPD test measure?
|
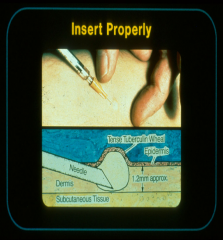
Measures the DTH response to PPD that screen for active and inactive TB cases. PPD is injected intra cutaneous
May show positive for foreigners who received different type of vaccine (BCG) |
|
|
When is a Tuberculin test measured? What constitutes a positive test? What is the follow up?
|
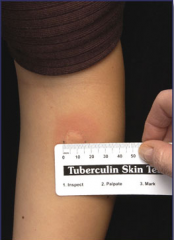
Measure 48-72H post injection
Measure diameter of induration, not erythema. A positive test is >10mm. It is also dependent on a proper DTH/CMI immune response (may not work in AIDs pts) Confirmationof a positive test is: CXR, clinical symptoms. Will be + if EVER infected |
|
|
Can a false negative occur for a TB test?
|
Yes, in the case that the pt is in the pre-DTH stage, Lost immunity to TB, Anergic, has AIDs or is Immunocompromised in any way.
|
|
|
What is a method of diagnosing TB from sputum? What is the sensitivity?
|
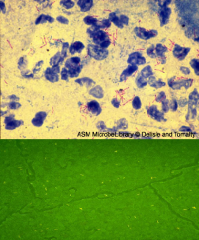
Top - acid fast stain of sputum is important (acid fast bacillus)
Bottom - fluorchrome stain showing yellow Mycobacterium TB organisms Only about 65% sensitive. |
|
|
What are the laboratory methods for diagnosing tuberculosis?
|
Culture on special media - 3+ weeks to culture. Often used to determine susceptibility.
Quantiferon gold TB test - measures IFN-gamma produced by T cells in while blood after 2 TB Ags are added to the blood. Measures active/latent TB. ($$$) RT-PCR from sputum and can detect rifamypin gene resistance too! Use giant rats |
|
|
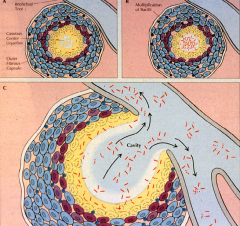
What is the pathogenesis of 1y and reactivation tuberculosis?
|

Tuberculosis. A. Primary tuberculosis. Mucobacterium tuberculosis is inhaled in droplet nuclei from an active case of tuberculosis. Initial multiplication is in the alveoli with spread through lymphatic drainage to the hilar lymph nodes. After further lymphatic drainage to the bloodstream, the organisms are spread throughout the body.
B. Alveolar macrophage. The two-front battle being carried out between A and C is shown. Ingested bacteria multiply in the nonactivated macrophage. (1) TH1 cellular immune responses attempt to activate the macrophage by secreting cytokines (interferon gamma [IFN-]). If successful, the disease is arrested. (2) Inflammatory elements of delayed-type hypersensitivity (DTH) are attracted and cause destruction. If activation is not successful, disease and injury continue. C. Reactivation tuberculosis. Reactivation typically starts in the upper lobes of the lung with granuloma formation. DTH-mediated destruction can form a cavity, which allows the organisms to be coughed up to infect another person. |
|
|
What is the epidemiology of mycobacterium tuberculosis? Transmission? dose, time, at risk populations & why?
|
p2p transmission
low infecting dose w/ long duration exposure At risk population: prison, low socioeconomic, nursing home, high population density & closed enviroment & absence of TB killing UV light, 50% new cases immigrants |
|
|
Describe histologically a tuberculous granuloma.
|

Tuberculous granulomas.
A. Early granuloma with lymphocytes, epithelioid cells and fibroblasts organizing around a central focus. The multinucleate giant cell in the center is typical of granulomas but not exclusive to Mycobacterium tuberculosis. B. Multiple granulomas surround and invade a vein near the lung hilum. Central degeneration is starting to appear and will eventually become caseous necrosis. |
|
|
Is Mycobacterium Tuberculosis susceptible? How is it treated in gen population? In healthcare workers w/ changed PPD test
|
Many multidrug resistant strains
Use multidrug regimens Treatment is multidrug until susceptibility is known and use DOTs (direct observed treatments) to increase adherence and decrease resistance formation Use INH prophylactically in skin convesion test in healthcare workers for 1year. |
|
|
What is the challenge in culturing mycobacterium tuberculosis?
|
Very slow growing - Doubling time 12-24H (due to complex cell wall). Culture may take 3-6wks and requires special media.
|
|
|
What is the immune response to Mycobacterium Tuberculosis?
|
DTH - destructive - NK cells recognize inactivated macrophages & kill them. This releases the mycobacteria and leads to granuloma formation
CMI - immune component - CD4/CD8 T cells & activated macrophages release INF-gamma which increases MHC1 expression. Humoral response little importance because intracellular pathogen |
|
|
How does a 1y TB infection heal?
|
Lesion (tubercle) heals by fibrosis
Microbe is slowly killed by activated Macrophages TB persists in aerated upper lobes w/ low lymphatic drainage |
|
|
What are the issues surrounding the TB vaccine?
|
BCG - effective only in children. Not really in adults
BCG is live attenuated vaccine of mycobacterium bovis Causes conversion of PPD which makes screening hard BCG not recomended in US |
|
|
What is miliary TB?
|
Disseminated TB infection. Name derives from CXR which resembles millet seed spread throughout the lungs.
Occurs as complication in 1-3% of cases. |
|
|
What are the symptoms of TB? A critical complication?
|
Cough, hemoptysis, night sweats & fever, weight loss (consumption)
CNS infection predominately in children (why give BCG vaccine) |
|
|
What mycobacterial species cause clinical manifestations similar to tuberculosis and how can these be differentiated from TB?
|
They are distinguished by biochemical rxns & characteristics (pigment formation)
Mycobacterial Avium - Clinically indistinguishable from mycobacterium TB. Major issue in AIDs pts. Mycobacterial Bovis - from unpasteurized milk. Causes GI TB, or lung TB if inhaled. Will cause +PPD test too! Mycobacteria Kansasii |
|
|
What is the epidemiology of Mycobacterium Leprae?
|
Generally not life threatening, just disfiguring & disabling.
Significant issue in developing nations |
|
|
What are the 2 extremes in the spectrum of clinical manifestation of Mycobacterium Leprae infections?
|
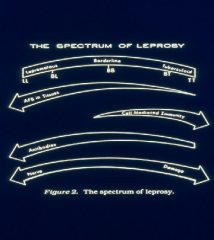
Lepromatous Leprosy - more severe
-Has low/no CMI response w/ poor development of granulomas. High # AFB in tissue & bloodstream, More contagious, High Ab levels Tuberculoid - minor severe Has CMI response to AFB granuloma, Few AFB in tissue, Low Ab, Rapid nerve damage, Not contagious (usually) |
|
|
What are the clinical manifestations of Lepromatous Leprosy?
|
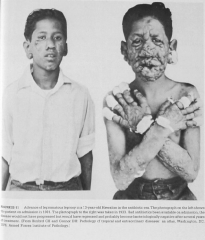
Slow deteriorating nerve damage -> anesthesia & loss digits & tissue damage & leonine facial features
------------------------------------ Lepromatous leprosy. Note the cutaneous plaques, infiltrates, and loss of eyebrows. Scrapings of the ear lobes would reveal numerous acid-fast bacilli. This advanced case will still respond to appropriate chemotherapy. |
|
|
How does the clinical manifestations and diagnosis similar and different in leprosy and tuberculoid?
|

They differ in strength CMI response, Ab levels, AFB counts, & contagious levels
--------------- Lepromatous leprosy (severe) - Loss of fingers due to not feeling wounds on the hands. |
|
|
What are the clinical manifestations of Tuberculoid leprosy?
|
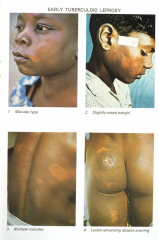
Tuberculoid - minor severe
Has CMI response to AFB granuloma, Few AFB in tissue, Low Ab, Rapid nerve damage (CMI response), Not contagious (usually) Anesthetic effect is localized. Later may lose motor function. |
|
|
What is the source and route of transmission of leprosy? Where is it cultured?
|

Humans are the ONLY resovoir and source of M Leprae (nasal discharge, break skin/mucous membranes, blood to skin/nerve)
Long incubation period Cultured in: mouse footpad armadillos |
|
|
What is the pathogenesis of M leprae?
|
M leprae is obligate intracellular parasite -> replicate skin macrophage & Schwann cells -> Chronic granulomatous disease of skin, peripheral nerves, & superficial tissue. -> peripheral nerves are invaded and anesthesia results.
|
|
|
How does the pathogenesis of M leprae in tuberculoid & lepromatous differ?
|
Tuberculoid has a strong CMI response -> contains infection to localized region -> Nerves are palpable and damaged leading to patches/lesions of anesthesized, hypopigmented & hairless skin
Lepromatous has weak CMI response -> uncontained microbe travels to cooler regions (face, nose, testis, extremities) -> More effected regions |
|
|
What is the bacteriology of Mycobacteria Leprae?
|
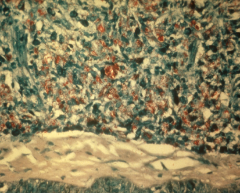
Weakly acid-fast bacillus
Obligate intracellular parasite Slow growing doubles in 11-13days Outer wall rich in mycolic acid Only grows in armadillos & mouse footpads ---------------------- High # of AFB Mycobacterium Leprae in tissue section |
|
|
What are the layers in order of the Mycobacteria cell wall?
|
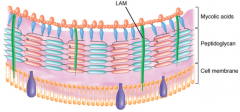
Cell membrane - Peptidoglycan Mycolic acids.
LAM, lipoarabinomannan. |
|
|
Summary of mycobacterium species
|

|
|
|
How are mycobacterium similar/different from other gram (+) organisms?
|
Differ in that high amounts of mycolic acid that makes it acid fast, hydrophobic
|
|
|
How is mycobacterium leprae diagnosed?
|
From acid fast smears of
skin slits/biopsies, nasal mucosa, ear lobe Lepramatous pts have high # AFB and are easier to dx. Tuberculoid pts may be dx clinically or through skin biopsies. |
|
|
How is mycobacterium leprae treated?
|
Tx is very effective & cheap
(multi to prevent formation of resistance) 1. Sulfones (dapsone) - some resistance from misuse 2. Rifampin 3. Clofazimine Tx should not be stopped even if rx reactions occur |
|
|
What is the source of tuberculosis like pathogens?
|
Environment
M. Bovis - unpasteurized milk M. Avium 0 birds, mammals in soil & water |
|
|
What is the importance of determining non mycobacterium tuberculosis- TB diseases?
|
They are generally harder to treat and have more Abx resistance.
|
|
|
What is another significant and frequent TB infection?
|
Mycobacterium Avium-Intracellular Complex (MAIC)
- A group of related AFB microbes that are very similar - Cause disease in adults, major issue in AIDs - Prognosis is grave when diagnosed with MAIC - Highly resistant & hard to treat |