Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
277 Cards in this Set
- Front
- Back
|
What are the two types of gametogenesis? What do they create?
|
- Spermatogenesis - male gamete (1N) = spermatozoon
- Oogenesis - female gamete (1N) = ovum |
|
|
What are the outcomes of gametogenesis?
|
- Mature gametes produced by meiosis + maturation
- Genetic diversity achieved by crossover as well as independent assortment of genes and random distribution of maternal and paternal chromosomes |
|
|
What is stored in the cytoplasm for continued development of the gametes?
|
mRNAs
|
|
|
What are the characteristics of a spermatozoon?
|
- 0.05 mm in length
- Designed to be mobile when mature w/ strong flagellum (travel at 22μm/sec) - Designed for penetration of the oocyte (mediated by enzymes released from acrosome) - Designed to deliver the paternal haploid genome |
|
|
What are the two varieties of sperm?
|
X and Y
|
|
|
How quickly can sperm reach the uterine tube?
|
5 minutes after placement in the vagina (moving at 22μm/sec)
|
|
|
What are the characteristics of an ovulated oocyte (ovum)?
|
- Large cell w/ abundant cytoplasm with organelles and nutritional reserves (0.1 mm in length, 2x sperm length)
- Designed for supporting and sustaining embryo development (stores important compounds in cytoplasm) - Divides after diploid chromosome number restored - Several coverings |
|
|
When can the oocyte divide by mitosis?
|
When diploid chromosome number (2N) is restored (after fertilization)
|
|
|
What are the coverings of the ovulated oocyte (ovum)?
|
- Outer layer: follicle / cumulus cells
- Acellular envelope, the zona pellucida (interlinked fibrous proteins) - Perivitelline Space - Oocyte cell membrane |
|
|
What is the zona pellucida made from?
|
Glycoproteins ZP 1, 2, and 3
|
|
|
What varieties do oocytes come in?
|
One - X
|
|
|
What are some causes of abnormal gametes?
|
- Morphological abnormalities (affect sperm and oocytes)
- Chromosomal abnormalities (errors of meiosis during gametogenesis) - Advanced parental age |
|
|
What are some causes of chromosomal abnormalities in gametes?
|
- Nondisjunction - can cause aneuploidies
- Translocations - from breakage and reunion of chromosomes - Deletions and microdeletions - missing segments of chromosomes - Fresh gene mutations |
|
|
What is more likely to happen with abnormal gametes?
|
- Birth defects
- Spontaneous abortion - Problems with infertility |
|
|
What is the average number of morphologically abnormal sperm in ejaculate? When is the percentage where the male may experience infertility?
|
- Average: 10%
- Infertility: 20-30% or higher |
|
|
What are some morphological problems that an oocyte might have?
|
- More than one nucleus
- Follicle with more than one oocyte |
|
|
What is the site of fertilization?
|
- Outer 1/3 of uterine tube (oviduct)
- AKA: ampulla - widest part of uterine tube |
|
|
Of the millions of sperm ejaculated, how many reach the ampulla?
|
Only a few hundred
|
|
|
How long are ovulated oocytes viable? Sperm?
|
- Oocytes viable for ~24 hours
- Sperm viable for 3-5 days in female reproductive tract |
|
|
What happens if an overripe ovum is fertilized?
|
Usually spontaneous abortion
|
|
|
What does the notations G#P# mean?
|
G# = number of pregnancies
P# = number of live births |
|
|
What is the journey of the sperm?
|
- In Male Reproductive Tract: Testis --> Epididymis --> Vas Deferens --> Ejaculatory Duct --> Urethra -->
- In Female Reproductive Tract: Vagina --> Uterus --> Oviduct (isthmus) --> Oviduct (ampulla) |
|
|
Where do sperm become motile?
|
Epididymis where they are stored until ejaculation
|
|
|
What kind of system is the male duct system? What are the implications of this?
|
Closed system - no barriers to transport
|
|
|
Once sperm enter the vagina, what barriers do they encounter?
|
- Vagina is very acidic; some women make antibodies to sperm
- Cervix mucosa is extremely folded providing many dead ends; also mucus consistency may be unfavorable for transport - May enter wrong oviduct - Isthmus of oviduct - sperm get detained for a few hours |
|
|
Where do sperm get detained on their way to the oocyte?
|
At the isthmus of the oviduct for a few hours
|
|
|
What is the journey of the oocyte?
|
- Short and rapid
- Presence of cumulus cells appears critical for oocyte pickup - Beating of cilia on cells lining oviduct and peristaltic contractions of muscular wall of oviduct move oocyte |
|
|
What are the steps of fertilization?
|
1. Capacitation
2. Binding of Sperm to Zona Pellucida (ZP) 3. Acrosome Reaction 4. Penetration of Zona Pellucida 5. Fusion of Sperm and Oocyte Cell Membranes 6. Oocyte Activation 7. Zygote Formation |
|
|
What happens during the first step of fertilization?
|
- Capacitation: final step in sperm maturation
- Activation of sperm at isthmus - Increases sperm metabolism and become capable of acrosome reaction - Become hypermobile - Become attracted to oocyte by unknown sperm chemotrophic factor |
|
|
What happens during the second step of fertilization?
|
- Binding of sperm to Zona Pellucida (ZP)
- Sperm receptors on ZP: ZP2 and ZP3 molecules - Acrosome intact sperm bind to ZP by SED1 (protein on sperm head surface membrane) |
|
|
If a sperm does not have an acrosome, can it bind to Zona Pellucida?
|
No - only acrosome intact sperm can bind to ZP because it has the SED1 membrane protein that binds to ZP2 and ZP3 receptors
|
|
|
What happens during the third step of fertilization?
|
- Acrosome reaction within seconds to minutes of binding to ZP
- Mediated by ZP2 and ZP3 - Sperm plasma membrane fuses with outer acrosomal membrane - Membrane vesicles that form are shed exposing acrosome enzymes - Involves Ca2+ mediated signaling pathways |
|
|
What happens during the fourth step of fertilization?
|
- Penetration of Zona Pellucida
- Acrosome enzymes (acrosin) hydrolyze ZP glycoproteins allowing sperm to pass through acellular protein coat - Movement of sperm tail facilitate ZP penetration |
|
|
What happens during the fifth step of fertilization?
|
- Fusion of sperm and oocyte cell membranes
- Once sperm enters perivitelline space it has access to oocyte cell membrane - Sperm plasma membrane at base of head is capable of fusing w/ oocyte membrane - Fertilinβ (ADAM2) on sperm membrane binds to an integrin (α6β1) on oocyte membrane - Protein on oocyte (CD9) modulates integrin binding - Sperm motility stops w/ fusion - Head, midpiece, and tail (usually) enter oocyte cytoplasm |
|
|
What kind of sperm can fuse with oocyte membrane?
|
Only sperm that have gone through acrosome reaction
|
|
|
What happens during the sixth step of fertilization?
|
- Oocyte Activation triggered by fusion of sperm and oocyte
- Initiates wave of intracellular Ca2+ --> transient hyperpolarization to block polyspermy - Cortical reaction - Ca2+ oscillations stimulate fusion of cortical granules w/ oocyte membrane --> hydrolytic and oxidative enzymes released into perivitelline space - Zona reaction - cortical granule enzymes enter ZP and crosslink ZP glycoproteins to prevent further sperm binding too by altering sperm receptor molecules - Meiosis completed - Ca2+ deactivates meiotic inhibitor - Male and female pronuclei form |
|
|
What is polyspermy? What are two ways that the oocyte prevents polyspermy?
|
- Entry of more than one sperm into oocyte, which can lead to polyploidy (lethal)
- Transient hyperpolarization of oocyte by wave of intracellular Ca2+ is an initial block of polyspermy - Zona reaction - cortical granule enzymes enter ZP and crosslink ZP glycoproteins to prevent further sperm binding by altering configuration of sperm receptor molecules |
|
|
How does the oocyte complete meiosis during oocyte activation (step 6 of fertilization)?
|
- Ca2+ ions deactivate meiotic inhibitor of oocyte
- 2nd polar body is extruded and a transient female pronucleus forms |
|
|
What is necessary for duplication of chromosomes?
|
Formation of male and female pronuclei
|
|
|
What happens during the seventh step of fertilization?
|
- Zygote formation
- Nuclear membrane breakdown of male and female pronuclei - Chromosomes form a metaphase plate - Now called a zygote (diploid) - Initiates first mitotic division |
|
|
How do you know that fertilization has occurred?
|
- Two pronuclei are in oocyte cytoplasm
- Two or three polar bodies are in the perivitelline space - Remnants of sperm flagellum in oocyte cytoplasm |
|
|
What are the results of fertilization?
|
- Oocyte completes meiosis
- Diploid chromosome number restored - genetic diversity generated by fusion of genomic material from two individuals - Sex is determined genetically (XX vs XY) - Next step in development (cleavage) is initiated |
|
|
Why are both parental genomes needed for conception?
|
- Male and female gametes are not equivalent
- Expression of the alleles of some maternal and paternal genes is not the same during embryonic development - Due to genomic imprinting |
|
|
What is genomic imprinting?
|
- Differential expression of male and female alleles of a gene
- Imprinting occurs during gametogenesis - Caused by differing methylations on DNA (methylation inactivates expression) - Therefore both sets of parental genes are necessary for complete development |
|
|
What happens if an oocyte with two paternal genomes and no maternal genomes forms?
|
Will form an intrauterine tumor called a hydatidiform mole (molar pregnancy)
|
|
|
How does genomic imprinting affect the insulin growth factor 2 (Igf2) gene?
|
- Male derived allele is expressed during embryonic development and in adult while female allele is silenced
- Female Igf2 receptor is expressed while male allele is silenced - Need both! |
|
|
How common is infertility in the U.S.?
|
15-30% of couples experience infertility
|
|
|
What are some methods of assisted conception for couples experiencing infertility?
|
- In Vitro Fertilization and Embryo Transfer (IVF-ET)
- Gamete Intrafallopian Transfer (GIFT) - Zygote Intrafallopian Transfer (ZIFT) - IntraCytoplasmic Sperm Injection (ICSI) |
|
|
What are the steps of In Vitro Fertilization and Embryo Transfer (IVF-ET)?
|
- Stimulate ovulation
- Collect oocytes - Obtain sperm - Capacitate sperm - Incubate gametes - Develop embryos to blastocysts - Implant blastocysts in uterus |
|
|
If 3 embryos are implanted using IVF-ET, what is the likelihood of success?
|
- 19% of IVF-ET attempts are successful
- 80% of successful implantations reach full term |
|
|
What is the weakest link in the In Vitro Fertilization and Embryo Transfer (IVF-ET) process?
|
Embryo transfer
|
|
|
What are side effects of In Vitro Fertilization and Embryo Transfer (IVF-ET)?
|
- Increased incidence of multiple pregnancies
- Spontaneous abortions and ectopic pregnancies - Increased incidence of birth defects (1.4-2x higher) |
|
|
What happens during Gamete Intrafallopian Transfer (GIFT)?
|
Gametes are collected and placed in the uterine tube
|
|
|
What happens during Zygote Intrafallopian Transfer (ZIFT)?
|
IVF produced zygote is placed into the oviduct
|
|
|
What happens during IntraCytoplasmic Sperm Injection (ICSI)?
|
In men experiencing infertility due to insufficient sperm count or abnormal sperm, a spermatozoon can be directly injected into the cytoplasm of an oocyte
|
|
|
The first three weeks of development are called what?
|
Embryogenesis
|
|
|
For the purpose of describing it, human embryonic development is traditionally divided into what two periods?
|
- Embryonic period (first 8 weeks)
- Fetal period (week 9 until birth) |
|
|
What is the timeline for the development of a zygote to a newborn?
|
38 weeks (266 days)
|
|
|
What happens during the embryonic period?
|
- Zygote (1 cell) --> Embryo (body plan, 3 layers, 3 axes)
- 3 Layers --> 4 tissues --> Organs and organ systems - Segmentation, head, limb and trunk formation, embryo folding |
|
|
What are the other two periods besides embryonic period and fetal period?
|
- Perinatal period (22 weeks to 1 month after birth)
- Neonatal period (birth to 1 month after birth) |
|
|
What developmental processes take place during the embryonic period (first 8 weeks)?
|
- Cleavage
- Blastocyst formation - Implantation - Differentiation - Germ layer formation - Segmentation - Axes definition - Embryo folding - Formation of body regions - Appearance of limbs - Establishment of body plan - Organogenesis |
|
|
How can the embryonic period be divided?
|
23 stages = Carneigie Stages
Characterized by observing surface changes in embryo as well as changes in size; recognizable stages overlap into a continuum |
|
|
What are the main features of the fetal period (week 9 to ~38 / birth)?
|
- Rapid body growth
- Maturation of many tissues and organs - Continued development of tissues and organs |
|
|
What are the two ages that can be used to describe the prenatal development?
|
- Fertilization age
- Gestational age |
|
|
When does the fertilization age begin and end?
|
- Begins with fertilization and ends at birth - true timing of human embryonic development
- No way to detect exact time of fertilization though - Usually 38 weeks |
|
|
When does the gestational age begin and end?
|
- Begins at the date of the last menstrual period and ends at birth
- Two weeks ahead of fertilization age - Usually 40 weeks |
|
|
How does gestation age compare to fertilization age?
|
Gestational age is 2 weeks ahead of fertilization age
|
|
|
If you are "15 weeks pregnant", how old is the fetus?
|
13 weeks old
|
|
|
What are the major events during the first week (days 1-6, stages 1-4) of embryonic development?
|
- Fertilization
- Cleavage - Blastocyst formation - Bilaminar embryonic disc formation - One cell --> solid ball of cells --> fluid filled cyst with disc |
|
|
How fast is the cell division during the first week of development? Do they all divide at the same time? How much are they growing?
|
- Rapid - every 12-24 hours
- No G1 or G2 - Divisions asynchronous - No cell growth (ratio of cytoplasm to nucleus goes from 600:1 --> 3:1 |
|
|
The bundle of cells that is formed after lots of cleavage during week 1 of development is called what?
|
Blastocyst - each cell is called a blastomere
|
|
|
Why is there no cell growth occurring during the first week of development?
|
Growth of the cleaving cell mass is restricted by Zona Pellucida (ZP)
|
|
|
What controls the first cell division during cleavage?
|
- A maternal program expressed and stored during oogenesis and activated during fertilization
- Embryo genome is activated at 2-4 cell stage |
|
|
What happens when embryo genome is activated?
|
- Paternally derived genes can now be expressed
- Proteins are needed to direct events occurring during cleavage and blastocyst formation |
|
|
What is meant by "constancy of the genome"?
|
- All cleavage stage blastomeres (cells of blastocyst) and eventually all nucleated cells of individual have same complete genome
- This is the biological basis of cloning |
|
|
What was determined in the Spemann experiment
|
- A nucleus from an early cleavage stage blastomere is capable of generating an entire embryo
- In mammalian embryos, each blastomere up to about the 8 cell stage has the potential to form a complete embryo if isolated and allowed to develop - If blastomere remains in place it only contributes to part of embryo |
|
|
At what point does the surface contact between adjacent blastomeres increase so that the individual borders become indistinct? What is this called?
|
Between 8 and 12/16 cell stage = compaction
|
|
|
What mediates compaction?
|
Increased expression of cell adhesion molecules (E-cadherin) on the blastomere plasma membrane
|
|
|
At the 12-16 stage what does the mass of blastomeres look like? What is it called?
|
Looks like a cluster of berries - called the Morula (mullberry)
|
|
|
What kind of cell sorting takes place at the 12-16 cell stage (morula)?
|
Some cells are inside and others are outside; sets up potential for formation of multiple cell lineages due to cell-cell interaction
|
|
|
At what stage does the ball of cells enter the uterus?
|
As a morula (12-16 cell stage)
|
|
|
On day four the blastomeres increase from 16-32 cells and forms what two cell lineages?
|
- Outer cells --> Trophoblast
- Inner cells --> Inner Cell Mass (ICM) aka embryoblast - Intercellular spaces appear between ICM cells and coalesce into single cavity (Blastocyst cavity) pushing ICM to one side |
|
|
When is the term blastocyst appropriate?
|
- When Trophoblast (outer cells) and Inner Cell Mass (ICM) form
- ICM pushes to one side to form the Blastocyst Cavity |
|
|
Which cells in the blastocyst are embryonic stem cells?
|
Inner Cell Mass (ICM) cells
|
|
|
What are the characteristics of the trophoblast?
|
- Outer layer of blastocyst
- First observable cell lineage of embryo - Flattened cells joined by cell junctions - Polarized (apical and basal surfaces) - Line blastocyst cavity - True epithelium |
|
|
What does the trophoblast form?
|
Only extraembryonic (chorionic) tissue
|
|
|
What controls the development of trophoblast tissue?
|
Subset of paternal derived and programmed genes (influenced by genomic imprinting)
|
|
|
What are the characteristics of the Inner Cell Mass (ICM)?
|
- Initially non-polarized
- Contribute to formation of embryo - Forms bilaminar disc (day 7) |
|
|
How is the bilaminar disc formed?
|
- From ICM cells on day 7
- ICM cells form a layer of cuboidal cells adjacent to blastocyst cavity --> lower layer called hypoblast (primary endoderm) - Remaining cells form upper layer called epiblast |
|
|
What do the cells of the epiblast form?
|
Mostly embryo and some extraembryonic tissue
|
|
|
The upper surface of the bilaminar disc indicates the future location of what?
|
Dorsal side of embryo
|
|
|
The lower surface of the bilaminar disc indicates the future location of what?
|
Ventral side of embryo
|
|
|
What is the first axis of symmetry to be visible in the embryo?
|
Dorsal-ventral polarity
|
|
|
What are the functions of the zona pellucida?
|
- Keep blastomeres together
- Provide an immunological barrier for blastocyst - Protect from premature implantation by preventing blastocyst-endometrium contact |
|
|
When is the blastocyst released from the Zona Pellucida? What does this allow?
|
Day 4-5 allows for implantation and an increase in size
|
|
|
What is believed to mediate the release of the blastocyst from the zona pellucida?
|
Enzymes released by the blastocyst
|
|
|
Cleavage stage embryos have potential for regulation, what does regulation mean?
|
Ability of an embryo/organ primordia to produce a normal embryo/structure when parts have been removed or added
|
|
|
How does the ability to regulate change as the embryo ages?
|
Decreased ability to regulate with age
|
|
|
What is meant by "todipotent"? When are cells "todipotent"?
|
- 0-8 cell stage
- Have all developmental pathway options and if isolated under appropriate conditions, could form a complete embryo |
|
|
What happens to the potency of cells in the 8-16 cell stage?
|
- Reduction in potency
- Trophoblast cells can only form trophoblast - ICM cells become multi- or pluripotent (multiple developmental pathway options) |
|
|
What genes allow ICM cells to maintain their pluripotent state?
|
Expression of genes Oct4, Nanog, Sox2, and CDH1
|
|
|
As cells age beyond 16 cell stage, what happens to their potency?
|
- Continues to reduce
- Ability of epiblast cells to regulate becomes further restricted and may eventually become bipotent or unipotent |
|
|
What does the term potency mean?
|
Full range of developmental capabilities available to a cell or embryo
|
|
|
What are chimeric embryos?
|
- Embryos that contain cells from more than one embryo and have cells with differing genotypes
- Can occur when two morula fuse during cleavage |
|
|
What is the impact of restricting developmental potency?
|
Leads to cell diversity
|
|
|
When a cell is limited to a specific developmental fate, it is called?
|
Cell differentiation
|
|
|
What is the end stage process of differentiation?
|
Terminal differentiation
|
|
|
What factors mediate differentiation?
|
- Cell position (external or internal)
- Number of cell divisions needed to restrict potency - Distribution of cellular messages (determinants) among blastomeres - Cell-Cell interactions |
|
|
Decisions about limiting a cell's potency are patterned and occur how?
|
By differential gene expression
|
|
|
What is "patterning" during development?
|
Recognizable, ordered, spatial arrangement that can occur at several levels, genes, cells, or tissues; often occurs along a particular axis or set of axes in embryo
|
|
|
What are some examples of gene families that control patterning? What kind of proteins do these code for?
|
- Homeobox (Hox)
- Paired box (Pax) - Pou - Code for DNA binding proteins or transcription factors |
|
|
What are homeotic mutations?
|
Examples of abnormal patterning during development
|
|
|
How are monozygotic twins formed?
|
Blastomere or inner cell mass separation
~65% formed by division at blastocyst stage ~35% formed by division between 2-cell stage to morula Very rarely, division occurs after formation of embryonic disc (can result in conjoined twins or parasitic twins) |
|
|
What percent of twins are monozygotic? Dizygotic?
|
- Monozygotic ~33%
- Dizygotic ~66% |
|
|
How are conjoined twins formed?
|
From incomplete separation of an embryo (1/50,000 of all twin births)
|
|
|
How common are twins?
|
1/90 births in USA
|
|
|
How do dizygotic twins form?
|
From a double ovulation and fertilization
|
|
|
What are the major events of the second week of embryonic development? What days and carnegie stages does it cover?
|
- Completion of impaction
- Amnion and umbilical vesicle formation - Extra-embryonic mesoderm formation - Days 7-12, Carnegie stages 4-6 |
|
|
What event bridges week 1 and week 2 of embryonic development? Which days?
|
- Impaction
- Days 5-12 (carnegie stages 4-5) |
|
|
What is necessary for impaction to be successful?
|
Development of embryo (free blastocyst) and endometrium of uterus (secretory phase of menstrual cycle) must be synchronized
|
|
|
What hormones influence the initiation of implantation?
|
Estrogen and progesterone from corpus luteum
|
|
|
What are the two phases of implantation?
|
- Attachment
- Penetration and embedment |
|
|
What happens during phase 1 of implantation?
|
- Blastocyst attaches to endometrium at the embryonic pole (side adjacent to ICM)
- Attachment is receptor mediated involving selectins and integrins - Triggers Decidual Reaction |
|
|
What is the Decidual Reaction? When does it occur?
|
- Phase 1 of implantation (attachment) - day 5
- Maternal reaction to and recognition of pregnancy - Endometrium thickens as stromal cells hypertrophy and blood flow to endometrium increases - Stromal cells accumulate glycogen and lipid causing glands to enlarge - Transforms outer 1/3 of endometrium into solid mass called "compact layer" |
|
|
What are the three layers of the endometrium during attachment of the blastocyst to the endometrium?
|
- Compact layer - part of functional zone - closest to uterine lumen
- Spongy layer - part of functional zone - Basal layer |
|
|
What happens during phase 2 of implantation?
|
- Penetration and embedment into the compact layer
- Formation of syncytiotrophoblast (ST); original trophoblast called the cytotrophoblast (CT) - Formation of lacunae |
|
|
What happens to the cells within the trophoblast when they contact the endometrium of the uterus?
|
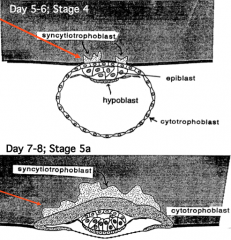
- Cells undergo mitosis
- Daughter cells form a multinucleated cytoplasmic mass with no observable intercellular boundaries = syncytiotrophoblast (ST) - Original trophoblast cells become the cytotrophoblast (CT) - By day 13 blastocyst is surrounded by ST and CT |
|
|
What controls the differentiation of the trophoblast?
|
- Integrins on trophoblast membrane
- Adhesive glycoprotein fibronectin and laminin - TGFβ may also be involved |
|
|
How does the blastocyst invade the endometrium of the uterus?
|
- Syncytiotrophoblast directs the enzyme mediated, controlled, invasion of the blastocyst into endometrium
- Cell membrane of ST contains abundant microvilli for absorption of nutrients from lysed decidual (compact layer) cells and eroded endometrial glands and blood vessels |
|
|
What are lacunae? When do they form?
|
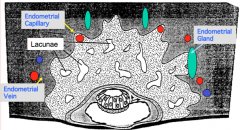
- During the penetration and embedment phase of implantation (day 9-12)
- Vacuoles or spaces appear within ST = lacunae - Spaces coalesce to form lacunar network - Maternal vessels and glands empty into them as they are eroded by ST |
|
|
At what point is the embryo fully embedded in the endometrium?
|
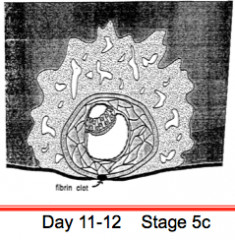
By day 11-12
|
|
|
What is the initial embryonic circulation?
|
Uteroplacental Circulation
|
|
|
What is secreted from the syncytiotrophoblast (ST) during implantation? What is its purpose?
|
Human Chorionic Gonadotrophin (hCG) - glycoprotein that maintains the corpus luteum in the ovary, which in turn, maintains the uterine endometrium
|
|
|
By what day can Human Chorionic Gonadotrophin (hCG) be detected in the urine (for a pregnancy test)?
|
By day 14
|
|
|
What are the potential sites of implantation?
|
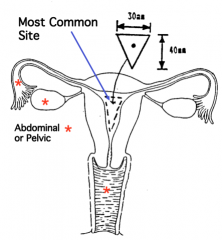
- Normally, inside the uterine cavity within the open triangular area
- Too close to the cervix (bad) - Outer 1/2 of oviduct (tubal pregnancy) |
|
|
What can happen if implantation occurs too close to the cervix?
|
- Placenta Previa (placenta detaches prematurely because endometrium here does not undergo decidual reaction)
- Less secure attachment |
|
|
What are the symptoms of a tubal pregnancy?
|
- Implants in outer 1/2 of oviduct
- Spotty bleeding - Acute, severe abdominal pain at 2.5 months - Vaginal bleeding |
|
|
What are some potential causes of tubal pregnancies?
|
- Any factor that prevents or retards the passage oft he zygote into the uterine cavity
- E.g., scarring from a tubal or paratubal infection, altered motility of tube or premature hatching of blastocyst from ZP |
|
|
How common are spontaneous abortions? What are some common causes?
|
- Estimated that 45-50% are miscarried
- Chromosomal abnormalities (~50%) - Homozygous lethal genes - Abnormal zygotes or problems with corpus luteum that leads to a failure to implant |
|
|
What structures are formed from the bilaminar disc?
|
- Amnion - forms in or above epiblast
- Umbilical Vesicle - Extraembryonic Mesoblast or Mesoderm - Chorion - Body Stalk |
|
|
How does the amnion form? What is the amnion?
|
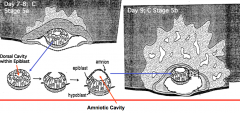
- Cells at the edges of the epiblast flatten and form a membrane around the cavity (around day 7-8)
- Cells are known as amnioblasts - Membrane formed is the amnion - extraembryonic membrane that will eventually surround the embryo and secrete amniotic fluid |
|
|
What are the functions of the amniotic fluid?
|
- Protects embryo and allows for symmetrical growth
- Allows for proper growth of lungs - Involved in fluid homeostasis - Allows for embryo movement - Helps control embryo body temperature |
|
|
How does the primary umbilical vesicle form? What is it?
|
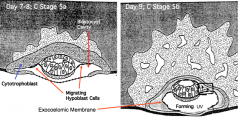
- Hypoblast cells at edge of embryonic disc flatten and migrate outwardly along the inner surface of the cytotrophoblast (CT)
- Form a membrane called the exocoelomic membrane - This membrane bounds a space called the primary umbilical vesicle (UV) aka yolk sac |
|
|
How does the secondary umbilical vesicle form? What happens to the primary UV?
|
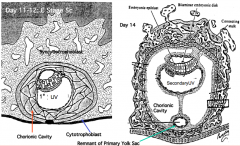
- Second group of flattened hypoblast cells migrate away from edges of embryonic disc
- Forms a smaller secondary umbilical vesicle (UV) aka yolk sac - Remainder of primary UV atrophies but may remain on opposite pole as small evesicles |
|
|
What is the function of the umbilical vesicle (UV) aka yolk sac?
|
- Metabolizes and transports nutrients from the trophoblast to embryo
- Site of initial blood and vascular formation - Primordial germ cells appear in wall as does hematopoiesis (formation of blood cells) - Portions become part of primitive gut |
|
|
What structure forms between the inner surface of the cytotrophoblast (CT) and the outer surface of the exocoelomic membrane?
|
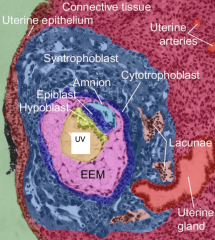
Extraembryonic mesoderm (EEM) aka mesoblast - a type of mesenchyme
(Shown in fuscia on picture) |
|
|
What do the Extraembryonic mesoderm (EEM) aka mesoblast cells form from?
|
From the exocoelomic membrane by delamination of cells (probably a type of epithelial-mesenchymal transformation)
|
|
|
What is mesenchyme?
|
- Non-polar, free cell derivative of embryonic epithelium
- Cells which are often motile - Second embryonic tissue type (1st - epithelial cells) - Ex: extraembryonic mesoderm (mesenchyme) forms from exocoelomic membrane (epithelial cells) |
|
|
Are mesoderm and mesenchyme the same thing?
|
No, not always interchangeable terms (however the extraembryonic mesoderm (EEM) aka mesoblast is a type of mesenchyme!)
|
|
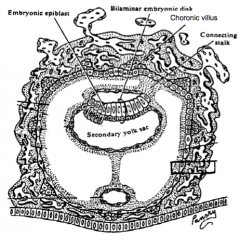
What is the term for the syncytiotrophoblast (ST), cytotrophoblast (CT), and extraembryonic mesoderm (EEM)? (Shown in black rectangle in picture)
|
Chorion
|
|
|
What are the solid clusters of cytotrophoblast (CT) that extend into the syncytiotrophoblast (ST)?
|
Primary chorionic villi
|
|
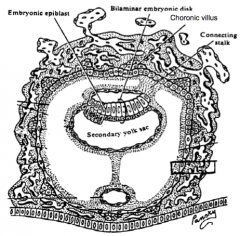
What is the space between the chorion and the extraembryonic mesoderm (EEM) coating the secondary UV (yolk sac)? (Shown as white spaces) What did it used to be called?
|
Chorionic cavity - formerly the extraembryonic coelom
|
|
|
When the extraembryonic mesoderm (EEM) accumulates between the chorion and the bilaminar disc, what does it form?
|
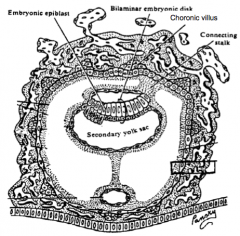
A bridge like structure - the connecting stalk
|
|
|
What does the connecting stalk do?
|
Connects the forming embryo to the chorion and will become the umbilical cord (blood vessels will form within body stalk)
|
|
|
What are the major events that occur during week three of embryonic development?
|
- Days 13-21 (stages 6/7-10)
- Trilaminar disc formation via gastrulation - Establishment of primary germ layers - Appearance of symmetry and asymmetry - Establishment of basic body plan - Beginning of organogenesis |
|
|
What is gastrulation?
|
Transformation from a bilaminar embryo to a trilaminar embryo
|
|
|
What are the steps of forming the three-layer embryo?
|
- Appearance of primitive streak
- Migration of the intraembryonic mesoderm - Formation of the notochord - Formation of oropharyngeal and cloacal membranes and the allantois - Establishment of symmetry and asymmetry |
|
|
How does the primitive streak form? Where is it located?
|
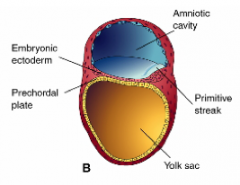
- Thickening of the epiblast with a midline groove due to converging epiblast cells
- As cells accumulate caudal to the streak, it elongates - At cranial end, the streak proliferates forming an elevated ridge called the primitive node - Near the connecting stalk |
|
|
What is the primitive node?
|
- Formed from cranial primitive streak cells proliferating to form an elevated ridge surrounding a small depression
- Important source for signaling molecules |
|
|
What happens to the epithelial cells on the primitive streak?
|
- Cells begin to transform from columnar cells to flask-shaped cells
- Flask-shaped cells lose polarity, detach from one another, and extend cell processes that contact the network of extracellular molecules (ECM) |
|
|
What happens to the transformed primitive streak cells?
|

Invagination - transformed cells slip beneath the epiblast
|
|
|
What is the term for the transformation that occurs at the primitive streak? What controls this?
|
- Epithelial-Mesenchymal Transformation (EMT) of converging epiblast cells
- Controlled by FGF8 secreted by cells of primitive streak |
|
|
What does FGF8 do during gastrulation?
|
- Controls cell migration, transformation, and specification of cells of primitive streak
- Causes a down regulation of cell adhesion molecule E-cadherin allowing epiblast cells to separate from each other |
|
|
Where do the first epiblast cells to transform invaginate? What do they form?
|
- Through primitive node (cranial end of primitive streak)
- Form definitive endoderm which replaces the hypoblast (primary endoderm) |
|
|
What do the epiblast cells that invaginate through the primitive node and primitive streak become?
|
- First to enter via primitive node --> Definitive Endoderm (replacing hypoblast cells) - form roof of umbilical vesicle / yolk
- Later cells entering via primitive node --> Prechordal plate - important for head and brain development - Primitive streak --> mesoderm cells (because they express Brachury gene) --> Intraembryonic Mesoderm (IEM) or mesoblast |
|
|
When the endoderm and mesoderm cells have invaginated through the streak, what are the remaining cells called?
|
Remaining epiblast --> Ectoderm
|
|
|
What are the three germ layer?
|
- Ectoderm
- Mesoderm - Endoderm ** All originated from epiblast |
|
|
After the intraembryonic mesoderm (IEM) has invaginated through the primitive streak, what do these cells do?
|
- Spread out between ectoderm and endoderm (b/c they are mesenchymal cells)
- Some migrate laterally while others travel cranially - Band of mesoderm (Septum Transversum) forms across cranial end of embryo - Expansion extends to edges of embryonic disc where cells of IEM become continuous w/ EEM |
|
|
Where does the notochord form from?
|

- Group of cells invaginate at primitive node and migrate toward opposite end of disc until encounter prechordal plate (at cranial end)
- These cells form the notochordal process between ectoderm and endoderm - Intercalate with cells of hypoblast forming a plate - As hypoblast is replaced by definitive endoderm, notochord cells detach and form solid cord of cells = notochord |
|
|
As the notochord is forming, what temporary communication appears?
|
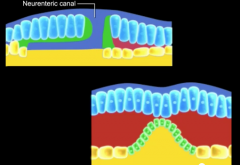
Neurenteric canal - between amniotic cavity and secondary UV (yolk sac)
|
|
|
What axis does the notochord go on to form?
|
Central cranial-caudal axis of embryo
|
|
|
What signaling is the notochord important for?
|
Signaling center for the dorsal-ventral patterning of the neural tube and smoites
|
|
|
What happens to the primitive streak?
|

- Becomes restricted to Tailbud region (caudal eminence)
- As notochord grows cranially, streak regress caudally, embryo lengthens along cranial-caudal axis - Eventually disappears by day 26-28 |
|
|
What are the two places where no mesoderm migrates between the fused ectoderm and definitive endoderm?
|
- Oropharyngeal membrane (at cranial end of trilaminar disc)
- Cloacal membrane (at caudal end of trilaminar disc) |
|
|
What is the function of the oropharyngeal membrane?
|
Separates future mouth and foregut
|
|
|
What is the function of the cloacal membrane?
|
Separates anus and hindgut
|
|
|
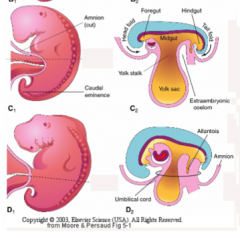
What is the diverticulum that pouches off of the umbilical vesicle (UV) aka yolk sac? Where does it go?
|
- Allantois - extends into body stalk
- Will later be surrounded by umbilical vessels - Remnant of allantois contributes to median umbilical ligament |
|
|
What is a teratoma?
|
- Remnants of primitive streak that form into a benign tumor
- Formed from multiple cell types - Most common type of tumor in newborns - Located in sacrococcygeal region - May be cystic or solid - Can be surgically removed with good prognosis |
|
|
What is a chordoma?
|
- Rare tumor formed from remnants of notochord
- Benign or malignant - 33% form at base of skull |
|
|
Where does an allantoic cyst form? Is it problematic?
|
- Extraembryonic portion of allantois where umbilical cord attaches to ventral body wall
- Usually asymptomatic unless they become inflamed or infected |
|
|
What is the condition "Caudal Dysgenesis" or "Sirenomelia"?
|
- Disruption of gastrulation
- Affects the lumbosacral spine, lower limbs, and urogenital system - May be caused by insufficient mesoderm production |
|
|
Expression of which genes establishes the cranial-caudal and dorsal-ventral axes of the embryo?
|
- Cranial-caudal: Otx2, Lim1, Hesx1
- Dorsal-ventral: chordin, noggin, follistatin, BrachuryT-FGF +BMP4 |
|
|
Expression of which gene initiates and maintains the primitive streak?
|
Nodal (member of TGF-β growth factor family)
|
|
|
Which genes are responsible for establishing left sidedness?
|
- Primitive node secretes FGF-8
- FGF-8 stimulates Nodal - Nodal accumulates in lateral mesoderm on left side of embryonic disc - FGF-8 also maintains expression of Lefty-2 - Node cells produce Lefty-1 (inhibits nodal expression on right side) - Nodal + Lefty-2 induce Pitx2 - Pitx2 in lateral mesoderm establishes left sidedness - Lefty-1 and Shh (sonic hedgehog) may prevent left sidedness factors on right side - Snail (transcription factor) restricted to right lateral mesoderm |
|
|
What happens if Lefty-2 is expressed on the right lateral mesoderm?
|
- Right sided heart (dextrocardia)
- Complete reversal of thoracic and abdominal organs (situs inversus) |
|
|
What are inductive cell or tissue interactions?
|
- Cell-cell interactions
- Cell-ECM interactions - Result from molecular signaling - Causes a modification of developmental fate for one or both participants (induction) |
|
|
What are the two components in an inductive interaction?
|
- Inducer - cell or tissue that is the source of the inductive signal
- Responder - cell or tissue that receives the inductive signal (must be competent to receive signal, i.e., must have proper receptors) |
|
|
How does the inductive signal arrive at the responder cell surface?
|
- Diffusion through ECM
- Can be locally or over a distance - If over a distance, a gradient of inducing signal may occur between source and responding cells - Sometimes inductive signal is passed from one cell to another by communicating junctions |
|
|
When does organogenesis begin?
|
End of week 3
|
|
|
What is morphogenesis? What cellular mechanisms mediate morphogenesis?
|
- Development of form
- Migration - Differentiation - Folding and expansion of cell layers - Proliferation - Programmed cell death - Epithelial-mesenchymal and mesenchymal-epithelial transformation - Cell-cell and cell-ECM interactions |
|
|
When does folding of the embryo begin? What does it establish?
|
- End of week 3
- Forms a tube-within-a-tube body plan |
|
|
What does the term "differential growth" refer to?
|
Some regions or areas of embryo grow fast while others may not grow at all or grow slower by comparison
|
|
|
What do the structures that are derived from the ectoderm do?
|
- Allow us to interact with the surrounding external environment
- Ex: epidermis (outer layer of skin) and nervous system |
|
|
What does the ectoderm develop into early on?
|
- Neuroectoderm
- Neural crest - Surface ectoderm |
|
|
Where do the signaling molecules come from that cause changes in the ectoderm?
|
- Notochord
- Prechordal mesoderm - Produce FGF which increases BMP4 antagonists noggin, chordin, and follistatin |
|
|
How dose the neuroectoderm form? What are these cells a precursor for? What is this process called?
|
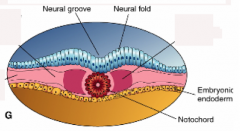
- Ectoderm on either side of midline thickens (neural folds / neural plate)
- Ectodermal cells get taller - Precursor of CNS - This transformation = Primary Neurulation |
|
|
What does the neural plate become?
|
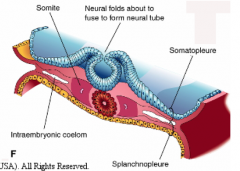
- Transforms into a neural tube
- Sides of neural plate elevate into neural folds - Folds appose each other and fuse to form tube - First fuse at area of 5th somite - continues cranially and caudally |
|
|
What are the neuropores?
|
The openings at the cranial and caudal ends so that the inner surface of the tube can access nutrients until blood vessels form; close by end of week 4
|
|
|
What does the cranial end of the neural plate eventually form?
|
Brain
|
|
|
During week 3, a ventral bend or flexure occurs in middle of expanded cranial end of neural tube, what are the areas surround it named?
|
- Prosencephalon / Forebrain - cranial to flexure
- Mesencephalon / Midbrain - at the flexure - Rhombencephalon / Hindbrain - caudal to flexure |
|
|
Where do the ear and eye primordia (earliest forms) appear?
|
- Otic disc - ectoderm thickening adjacent to rhombencephalon / hindbrain - forms inner ear
- Optic sulcus - groove appears on either side of prosencephalon / forebrain - forms eyeball |
|
|
How does the neural crest form?
|
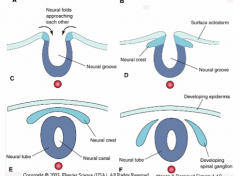
- Cells on lateral edge of neural folds undergo an epithelial-mesenchymal tranformation
- These cells migrate or are displaced from neuroectoderm |
|
|
What are the neural crest cells precursors for?
|
- Primary sensory neurons
- PNS sheathing cells - Neurons of autonomic ganglia - Pigment cells |
|
|
What happens to the ectoderm that does not become neuroectoderm?
|
- Becomes surface ectoderm
- Continues to express high BMP4 - Becomes epidermis of the skin |
|
|
What are the three regions of intraembryonic mesoderm?
|
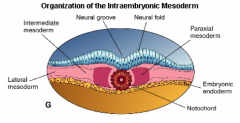
- Paraxial mesoderm
- Intermediate mesoderm - Lateral mesoderm (Notochord is considered the "axial mesoderm") |
|
|
What are the characteristics of the paraxial mesoderm in the head and the trunk?
|
- Head - remains unsegmented - known as Head Mesoderm
- Trunk - becomes segmented (subdivisions = somites) |
|
|
What are somites made from?
|
- Subdivisions of trunk paraxial mesoderm
- Transient structures that allow for further organization of mesoderm derived precursor cells |
|
|
How many pairs of somites form by the end of week 5? How are the somite pairs classified?
|
42-44 pairs total
- 4 occipital - 8 cervical - 12 thoracic - 5 lumbar - 5 sacral - 8-10 coccygeal - Not all present at same time because cranial pairs begin to differentiate further and disassociate before caudal most somite pairs form |
|
|
How is the appearance of somites mediated?
|
- By molecular segmentation clock
- Periodic appearance - Segmentation of presomite area - Increase in "Notch" expression leads to segment patterning genes to establish a new pair |
|
|
How are the somite boundaries established?
|
- Cranially by retinoic acid
- Caudally by FGF and Wnt3a |
|
|
What happens to the mesenchyme of the forming somites?
|
- Undergoes a mesenchymal to epithelial transformation
- Epithelial cells arrange around a lumen called the somatocele |
|
|
Where is the intermediate mesoderm located? What does it become?
|
- Lateral to paraxial mesoderm
- Form a solid cord of mesenchyme cells along back wall in trunk = nephrogenic ridge - Tissue eventually differentiates into gonads and kidneys = urogenital ridge |
|
|
Where is the lateral mesoderm located? What does it become?
|
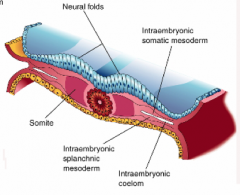
- Lateral to intermediate mesoderm
- Intercellular spaces coalesce forming intraembryonic ceolom (inverted U shape - connected cranially) - Ceolom splits lateral mesoderm - One layer associates with ectoderm = somatic mesoderm - One layer associates with endoderm = splanchnic mesoderm |
|
|
Which region of mesoderm becomes the somatic mesoderm and splanchnic mesoderm?
|
Lateral Mesoderm - after being split by the intraembryonic coelom
|
|
|
What is the name for the ectoderm + lateral plate mesoderm?
|
Somatopleure
|
|
|
What is the name for the endoderm + lateral plate mesoderm?
|
Splanchnopleure
|
|
|
What are the precursors of the cardiovascular system called?Where does it begin?
|
Hemeangioblasts - begins in wall of umbilical vesicle (UV) aka yolk sac
|
|
|
Where are the first blood vessels found? What do they form from?
|
- Wall of umbilical vesicle (UV) aka yolk sac
- Form from precursor cells called angioblasts by vasculogenesis |
|
|
How do the heart and aorta form?
|
- Via vasculogenesis from angioblast (precursor cells)
- In anteriolateral regions of splanchnic mesoderm associated with transverse part of embryonic coelom |
|
|
Once the initial vessels form, how do the remaining vessels develop?
|
Primarily as vascular buds or branches from existing vessels via angiogenesis
|
|
|
The tube-within-a-tube plan is composed of what layers?
|
- Outer tube = ectoderm
- Inner tube = endoderm |
|
|
How does the tubular embryo form from a flat, trilaminar embryo?
|
Folding of the embryonic disc in Sagittal and Trasnverse planes
|
|
|
What are the effects of folding the embryo in the sagittal plane along the cranial-caudal axis?
|
- Flat embryo becomes C-shaped (head-fold and tail-fold bend inward)
- Embryo lifted up into amniotic cavity |
|
|
What is the major driving force for folding along sagittal plane / cranial-caudal axis?
|
Neural tube elongation
|
|
|
What forms the "head fold"? What does this result in?
|
- Extension of the neural tube cranially beyond the oropharyngeal membrane
- Results in relocation of several structures from dorsal to ventral including septum transversum (forming heart tube, pericardial part of coelom, and oropharyngeal membrane) |
|
|
What forms the "tail fold"? What does this result in?
|
- Extension of neural tube caudally beyond cloacal membrane
- Results in cloacal membrane, connecting stalk, and allantois relocating from dorsal to ventral positions |
|
|
What forms the foregut and the hindgut?
|
Part of UV endoderm
|
|
|
What is thought to drive folding in the transverse plane?
|
- Expansion of somatopleura (ectoderm + somatic mesoderm)
- Expansion of amnion - Formation of somites may contribute - Elongation of neural tube may also contribute by causing lateral folds to bend downward |
|
|
What is the result of folding in the transverse plane?
|

- Formation of outer tube of surface ectoderm
- Formation of inner tube of endoderm --> primitive gut: foregut, midgut, and hindgut |
|
|
What does the midgut communicate with?
|
Umbilical vesicle via the omphaloenteric or vitelline duct
|
|
|
How is the gut tube suspended from the body wall?
|

Mesentery
|
|
|
What are the four body folds?
|
- Head fold
- Tail fold - 2 x Lateral folds |
|
|
The four body folds are continuous domains of a common circle that converge to form what?
|
Umbilical ring / connecting stalk
|
|
|
When does the fourth week of embryonic development happen?
|
Days 22-28, stages 10/11-13
|
|
|
What are the characteristics of the embryo at the beginning of the 4th week?
|
- Heart is beating
- Embryonic circulation is established and connected to yolk sac and placenta - Neural tube is mostly closed but open at each end Folding of embryo has begun - Somite pairs continue to form - Embryo is ~2 mm in length (will grow to about 5 mm this week) - Chorionic sac is 2 mm in diameter (will increase to 3.5 mm ~size of BB) |
|
|
Where does the intraembryonic coelom appear and when?
|
- Appears as spaces within the lateral plate mesoderm
- Late in the third week |
|
|
What is the somatic mesoderm continuous with?
|
Extraembryonic mesoderm coating the amnion
|
|
|
What is the splanchnic mesoderm continuous with?
|
Mesoderm that coats the umbilical vesicle (yolk sac)
|
|
|
What shape does the intraembryonic coelom take?
|
U-shaped space by early in 4th week
|
|
|
What are the legs of the "U-shaped" intraembryonic coelom called?
|
Pericardioperitoneal (Pleural) Canals
|
|
|
What is the transverse part of the "U-shaped" intraembryonic coelom called? Which end is it on (cranial/caudal)?
|
Primitive Pericardial Cavity - cranial end but caudal to septum transversum
|
|
|
After folding the embryo in the sagittal plane, what are the relationships of the intraembryonic coelom?
|
- Transverse portion (primitive pericardial cavity) is ventral to the longitudinal portions (pericardioperitoneal (pleural) canals)
- Pericardial cavity is median and ventral to pleural cavities that are more lateral and dorsal |
|
|
After folding the embryo in the horizontal plane, what are the relationships of the intraembryonic coelom?
|
- Longitudinal portions of coelom (pericardioperitoneal (pleural) canals) approach each other
- Become ventral to neural tube and surround primitive gut tube |
|
|
What are the longitudinal portions of the intraembryonic coelom continuous with laterally, initially?
|
Extraembryonic Coelom (aka Chorionic Cavity) - this connection is lost when the ventral body wall forms during the folding of the embryo in horizontal plane
|
|
|
What is the septum transversum?
|
- Wedge, or semicircular shelf, of mesenchyme derived from intraembryonic mesoderm
- After embryo folds in sagittal plane, it is located to caudal to forming heart, ventral to presumptive pleural cavities, and cranial to presumptive abdominal cavity - Partial partition, incompletely dividing the intraembryonic coelom into a cranial thoracic portion and a caudal abdominal portion |
|
|
What does the septum transversum contribute to forming?
|
Diaphragm
|
|
|
As the embryo folds in the horizontal plane, the abdominal portion of the primitive gut tube becomes suspended from what?
|
Back wall of embryo by a double-layered dorsal mesentery
|
|
|
What structure is attached to the foregut and organs derived from it? Which organs?
|
Ventral mesentery - stomach, liver, part of esophagus, and part of duodenum
|
|
|
What lines the intraembryonic coelom?
|
- Lateral plate mesoderm split into two layers by coelom formation
- Parietal layer (from somatic mesoderm) lines wall of the coelom cavity - Visceral layer (from splanchnic mesoderm) covers organs extending into cavity |
|
|
At what point are the parietal and visceral serous membranes continuous?
|
Continuous at dorsal mesentery and the hilum of the leg
|
|
|
What does the epithelium covering the serous membranes secrete? What is its purpose?
|
Protein rich, watery or serous fluid - moistens the membranes and allows them to smoothly glide over each other when in contact
|
|
|
Which body wall fold is most likely to fail to close?
|
Lateral body wall folds due to insufficient migration of folds ventrally or a fusion problem or possibly re-rupture of previously fused folds
|
|
|
What are some examples of ventral body wall defects?
|
- Ectopic Cordis (externalized heart)
- Cantrell Pentalogy - Gastroschisis (externalized bowel) - Bladder and Cloacal Exstrophy (externalized bladder) |
|
|
Where is the cardiogenic crescent located?
|
- Within the splanchnic mesoderm forming the medial wall of the primitive pericardial cavity (transverse portion of intraembryonic coelom)
- Bulges into primitive pericardial cavity as it forms - Cranial to septum transversum |
|
|
What causes the pericardioperitoneal canals (longitudinal portions of U-shaped coelom) to become separated from the primitive pericardial cavity (transverse portion)?
|
Pleuropericardial folds expand and fuse with the mesenchyme ventral to the foregut
|
|
|
Where do the lung buds grow from?
|
- Dorsal to primitive pericardial cavity
- Laterally from the respiratory diverticulum (derivative of foregut) |
|
|
What two portions does the expansion of the forming lungs split the body wall into?
|
- Definitive body wall
- Pleuropericardial Folds |
|
|
What are the pleuropericardial folds?
|
- Small ridges in wall of coelom
- Expand to fuse with mesenchyme ventral to foregut - Forms a partition between the pericardial cavity and paired pleural cavities |
|
|
What is found within the pleuropericardial folds?
|
- Common Cardinal Veins
- Phrenic Nerves |
|
|
Where do the phrenic nerves originate? Where do they end up?
|
- Originate in pleuropericardial folds
- End up in pericardium |
|
|
After being separated from the pericardial cavity, the pericardioperitoneal canals remain open caudally with what?
|
The forming abdominal cavity
|
|
|
What projects into the caudal end of the pericradioperitoneal canals?
|
Crescent-shaped pleuroperitoneal folds
|
|
|
As the forming lungs grow, what happens to the pleuroperitoneal folds?
|
The folds are drawn out to form pleuroperitoneal membranes that will fuse with the mesentery dorsal to the forming esophagus
|
|
|
What closes the connection between the pleural cavities and the abdominal cavities?
|
The fusion of the plueuroperitoneal membranes with the mesentery dorsal to the forming esophagus
|
|
|
What forms the costodiaphragmatic recesses?
|
The expansion of the lungs into the body walls, enlarging the pleural cavities
|
|
|
What does the diaphragm separate?
|
- Thoracic cavity
- Abdominal cavity |
|
|
What does the diaphragm form from?
|
Merger of 3 primordia: septum transversum, dorsal mesentery of esophagus, and paired pleuroperitoneal folds
|
|
|
How is the fusion of the pleuroperitoneal membranes with the mesentery dorsal to the esphagus and septum transversum differ on each side?
|
The left membrane is larger and fuses later than the right membrane
|
|
|
Mesenchyme that forms on the peripheral rim of the pleuroperitoneal membranes is invaded by what? What does this do?
|
Myoblasts - muscle forming cells - form muscular portion of diaphragm
|
|
|
What is the diaphragm innervated by?
|
Phrenic Nerve
|
|
|
What does the septum transversum form on the diaphragm?
|
Central tendon of the diaphragm
|
|
|
Where do the crura of the diaphragm develop?
|
Within the mesentery dorsal to the esophagus
|
|
|
Where does the septum transversum originate and end up?
|
- Originates adjacent to cervical somites 3, 4, and 5
- Descends past thoracic somites because of the rapid growth of the dorsal part of the embryo (including the neural tube and vertebral column) - Eventually extends caudally to the level of the first lumbar vertebra |
|
|
What is the most common defect of diaphragm formation?
|
Posterolateral Defect of the Diaphragm - usually unilateral (left side most common) - caused by an incomplete formation/fusion of the pleuroperitoneal membrane with the septum transversum
|
|
|
If the pleuroperitoneal membrane fails to fuse with the septum transversum, what can happen?
|
- Leaves a posterolateral opening between the thoracic and abdominal cavities
- Through this defect the abdominal organs can herniate into the thoracic cavity - This is called Congenital Diaphragmatic Hernia (CDH) |
|
|
What are the most common organs involved in a Congenital Diaphragmatic Hernia (CDH)?
|
- Stomach
- Spleen - Intestines - Occasionally the liver |
|
|
What is the most common cause for pulmonary hypoplasia? What are the implications of this disease?
|
- Congenital Diaphragmatic Hernia (CDH)
- Often is fatal due to persistent pulmonary hypertension - Heart and mediastinum are often shifted to the right - Abdomen becomes narrow and anterior wall is sunken (= "scaphoid abdomen") - Polyhydramnios (excess amniotic fluid) |