![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
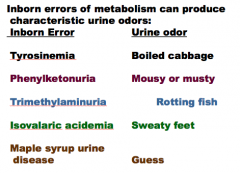
Inborn Errors of Metabolism:
Commonly involve the metabolic factory, |
Commonly involve the metabolic factory, |
|
|
What is the urine smell of each?
Tyrosinemia Phenylketonuria Trimethylaminuria Isovalaric acidemia Maple syrup urine disease
Smell: Mousy or musty Maple syrup Sweaty feet Boiled cabbage Rotting fish |
|
|
|
How do you diagnose tyrosinemia? |

|
|
|
|
|
|
“Inborn errors of metabolism of a given pedigree Family history is important, esp. _____, _____ history is important because specific Poor feeding + lethargy + seizures suggests Older children may present with _____ |
“Inborn errors of metabolism of a given pedigree Family history is important, esp. consanguinity, Dietary history is important because specific Poor feeding + lethargy + seizures suggests Older children may present with EPISODIC |
|
|
INBORN ERRORS OF METABOLISM Helpful tests: ammonia, _____, pH, glucose, If ammonia, bicarbonate and pH all _____, In episodic disease, lab tests can normalize If diagnosis unclear and liver biopsy done, |
INBORN ERRORS OF METABOLISM Helpful tests: ammonia, bicarbonate, pH, glucose, If ammonia, bicarbonate and pH all normal, In episodic disease, lab tests can normalize If diagnosis unclear and liver biopsy done, |
|
|
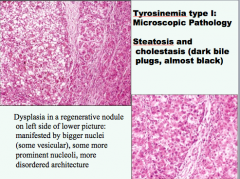
Tyrosinemia type I Aminoacidopathy due to Backup of metabolism of _____ leads to Liver toxicity manifested by _____, |
Tyrosinemia type I Aminoacidopathy due to Backup of metabolism of tyrosine leads to Liver toxicity manifested by steatosis, |
|
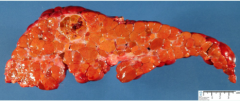
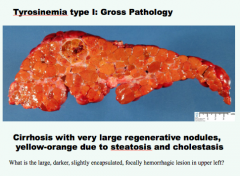
What is the gross pathology for tyrosinemia type I? |
|
|
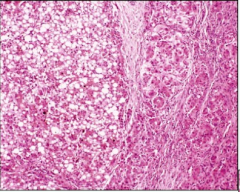
Steatosis, cholestatis (dark bile plugs, almost black). Diagnosis? |
|
|
|
Tyrosinemia type I:
Classic presentation: in first few months of life: |
Tyrosinemia type I Classic presentation: in first few months of life: |
|
|
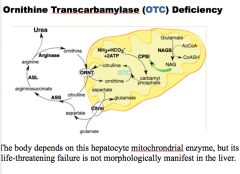
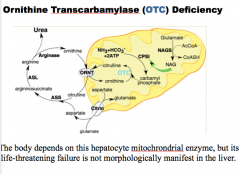
Ornithine Transcarbamylase (OTC) Deficiency The most common _____ cycle disorder |
Ornithine Transcarbamylase (OTC) Deficiency The most common urea cycle disorder |
|
|
|
|
|
GAUCHER’S DISEASE ___________ adult form = the most common autosomal __________, |
GAUCHER’S DISEASE beta-glucocerebrosidase adult form = the most common autosomal recessive, |
|
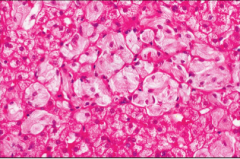
Kupffer cells and macrophages with expanded crinkled cytoplasm. Diagnosis? |
Gaucher's disease |
|
|
GAUCHER’S DISEASE ________= most common initial sign, Other manifestations: pancytopenia, bone pain Diagnosis by assay of __________e in white blood cells Treatment: enzyme replacement |
GAUCHER’S DISEASE Splenomegaly = most common initial sign, Other manifestations: pancytopenia, bone pain Diagnosis by assay of beta- Treatment: enzyme replacement |
|
|
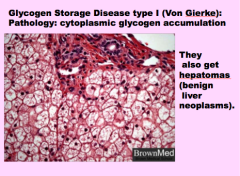
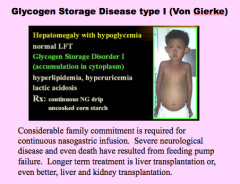
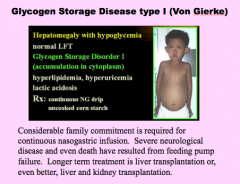
Glycogen Storage Disease type I (Von Gierke) Deficiency of ________, |
Glycogen Storage Disease type I (Von Gierke) Deficiency of glucose-6-phosphatase, |
|
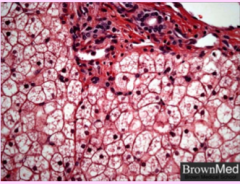
Cytoplasmic glycogen accumulation. Diagnosis? |
|
|
|
|
|
|
What is a diverse group of inverse errors of metabolism involving enzymes in heme synthesis (not all in bone marrow, 20% in liver)?
What are the two subgroups? |
Porphyrias
Acute and subcutaneous |
|
|
What is the most common porphyria? When does it present? Common presentation (skin and mechanism that follows)? |
|
|
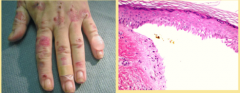
What is shown here? How do these lesions heal? |

|
|
|
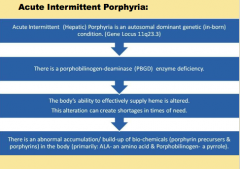
What is the acute intermittent porphyria mechanism? |
|
|
|
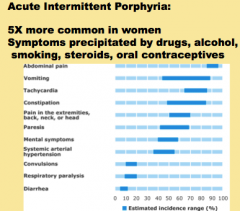
Acute intermittent porphyria: Most common in which sex? Symptoms precipitated by which five things? |
|
|
|
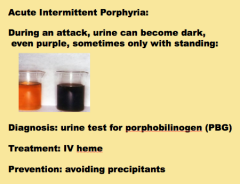
How do you diagnose acute intermittent porphyria?
What is the treatment?
How do you prevent?
|
|
|
|
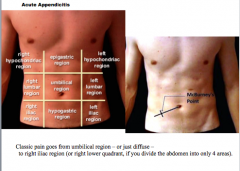
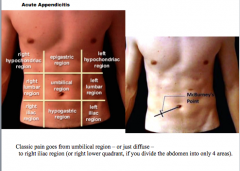
Epidemiology of what disease? |
Acute appendicitis |
|
|
Draw the pathway of acute appendicitis pathogenesis: |
Pathogenesis: thought to be initiated by progressive increases in intraluminal |
|
|
Pathology of appendicitis: In early acute appendicitis _____ vessels are congested and |
Pathology: In early acute appendicitis subserosal vessels are congested and |
|
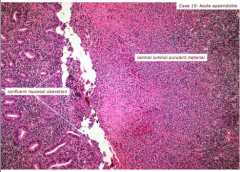
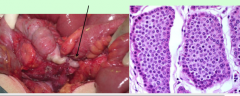
What is shown here? |
Acute appendicitis |
|
|
Classic presentation: periumbilical pain that gradually localizes A classic physical finding is the McBurney sign,
CLASSIC PRESENTATIONS AND FINDINGS FOR WHAT? |
Acute appendicitis |
|
|
Classic signs and symptoms of acute appendicitis are often absent: In some cases, a ______ appendix may generate right flank or pelvic pain, As with other causes of acute inflammation there is ______ leukocytosis, The diagnosis of acute appendicitis in young children and the very old is |
Classic signs and symptoms of acute appendicitis are often absent. In some cases, a retrocecal appendix may generate right flank or pelvic pain, As with other causes of acute inflammation there is neutrophilic leukocytosis, The diagnosis of acute appendicitis in young children and the very old is |
|
|
|
|
|
What are five things that a diagnosis of acute appendicitis be confused with? |
1. Mesenteric lymphadenitis (secondardy to unrecognized Yersinia infection or viral enterocolitis) 2. Ectopic pregnancy 3. Acute salpingitis 4. Mittelschmerz (pain cause by minor bleeding at time of ovulation) 5. Meckel diverticulitis |
|
|
What are the five complications of acute appendicitis? |
Complications of appendicitis include (1) perforation*, (2) peritonitis, |
|
|
If you can only remember one differential diagnosis and one complication from acute appendicitis, what should you remember? |
Mesenteric lymphadenitis (children) Ectopic pregnancy (adults)
Perforation |
|
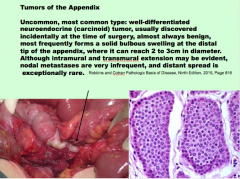
What is shown here? Common/uncommon? What tumor type? Benign/malignant? What part of appendix? |
|
|
|
Tumors of the Appendix:
Conventional adenomas or _____ producing Mucocele, a dilated appendix filled with _____, may simply |
Tumors of the Appendix Conventional adenomas or non–mucin-producing Mucocele, a dilated appendix filled with mucin, may simply |
|
|
Pyloric Stenosis Uncommon, but up to 0.35% of live births Classic presentation __- to __-week-old baby |
Pyloric Stenosis Uncommon, but up to 0.35% of live births Classic presentation 3- to 6-week-old baby |
|
|
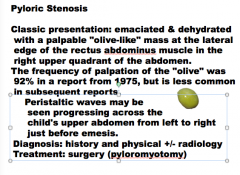
What is the classic presentation of pyloric stenosis?
What is the size of the palpable nodule?
What can you see progressing across the child's upper abdomen from left to right just before emesis?
What is the treatment? |
|
|
|
Differential for vomiting in an infant?
|
|