Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
211 Cards in this Set
- Front
- Back
|
What are nerves?
|
-bundles of nerve fibers (axons) outside the central nervous system +connective tissue binding them together + blood vessels (vasa nervorum) to supply them with oxygen, nutrients, & removal of carbon dioxide
|
|
|
How to classify nerves?
|
1. exit from bony encasement of CNS (cranial vs spinal)
2. function of the majority of contained fibers (motor-efferent vs sensory-afferent) 3. derivation from single or multiple spinal cord segments (segmental vs peripheral) 4. destination of contained fibers (somatic vs visceral) |
|
|
Cranial nerves
|
-exit cranial cavity via openings (foramina) in cranium (skull)
-12 pairs, identified by name, roman numeral, or both -all but one (spinal accessory) arises from brain -purely sensory, purely motor, or mixed |
|
|
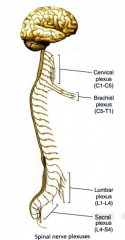
Spinal nerves
|
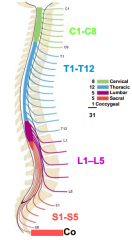
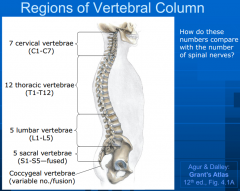
-exit from vertebral column (spine)--intervertebral foramina
-Identified by letter (indicating region) and number -31 pairs: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal |
|
|
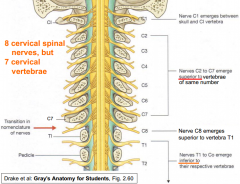
Numbering of spinal nerves
|
|
|
|
Function of the majority of the contained fibers:
|
-Sensory nerve: any nerve coursing in the subcutaneous tissue (e.g. the cutaneous branches of the dorsal rami of thoracic nerves)
-Motor nerve: a nerve to a skeletal muscle (e.g. spinal accessory nerve) |
|
|
Somites
|
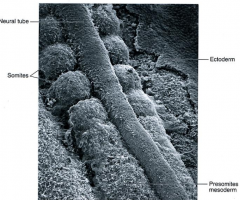
-segmented structure of our bodies.
-during somite period of development, tissue somites in pairs -each pair gives rise to the muscle, skin and bones/joints supplied by a single (rt. & left) pair of spinal nerves |
|
|
Sclerotomes
|
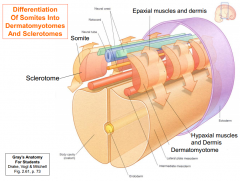
Medial sides of somites become sclerotomes, cells of which exit the somite and migrate medially.
-Differentiation of somites into dermatomyotomes and sclerotomes -ventrally migrating cells surround the notochord forming the beginnings of vertebral bodies -dorsally migrating cells surround the neural tube forming the beginnings of the neural arch of the vertebrae |
|
|
Dermatomyotomes
|
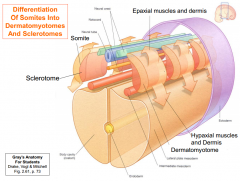
-give rise to the skeletal muscles and dermis of the skin of the trunk and limbs
-cells of the dermatomyotome that migrate posteriorly give rise to the intrinsic or epaxial (deep) muscles of the back and overlying dermis |
|
|
Motor neurons
|
-develop within the anterior neural tube send processes peripherally into the posterior and anterior regions of the dermatomyotome
-motor nerve fibers service a specific dermatomyotome continue to innervate muscles that develop from it. |
|
|
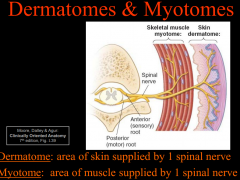
Myotome
|
muscle mass innervated by single spinal cord segment or, on one side, by a single spinal nerve
|
|
|
Sensory neurons
|
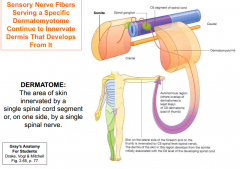
-Somatic sensory neurons send afferent fibers into dermatomyotomes
-sensory neurons developing within neural crests send peripheral processes into these regions of myotome, and central processes into the posterior neural tube. -sensory nerve fibers can serve specific dermatomyotome, these nerves continue to innervated dermis that develops from it. |
|
|
Motor and sensory nerves
|
-somatic sensory and motor nerve fibers are organized segmentally along neural tube. these all become parts of all spinal nerves and some cranial nerves
-clusters of sensory cell bodies are derived from neural crest, located outside CNS, form sensory ganglia |
|
|
Dermatomes & myotomes
|
|
|
|
Dermatomes
|
-area of skin supplied by a single spinal nerve is called dermatome
|
|
|
Herpes zoster (shingles)
|
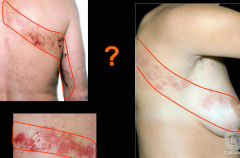
-virus resides in ganglion of spinal nerve.
-Affected dermatome develops rash |
|
|
What composes the roots of spinal nerves?
|
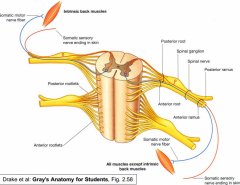
1. Posterior (dorsal) roots
2. Anterior (ventral) roots |
|
|
Posterior (dorsal) roots
|
-Afferent (sensory) only
- pseudounipolar neurons - cell body in spinal sensory (posterior or dorsal root) ganglion -single process divides into peripheral (extends to sensory nerve terminal) and central process (enters CNS) |
|
|
Anterior (ventral) roots
|
-efferent (motor) only
-multipolar neurons (have a receiving dendrite and sending axon end) -cell body lies within CNS |
|
|
Posterior and anterior roots in perspective
|
* posterior and anterior roots are only site where the functional components (afferent, efferent fibers) of spinal nerves are separable.
|
|
|
Injury to posterior root?
Injury to anterior root? |
posterior- loss of sensation (anesthesia)
anterior- loss of motor function (paralysis or palsy) |
|
|
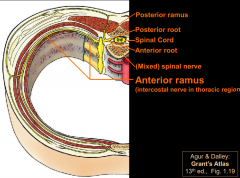
Rami (branches) of spinal nerves
|
-as soon as roots unite to form (mixed: motor and sensory) spinal nerve, it divides into two major branches (rami)
-posterior ramus and anterior ramus |
|
|
Posterior Ramus
|
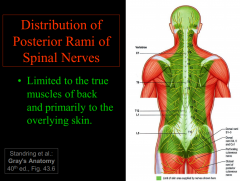
- turns sharply posteriorly around vertebral column, supplying:
-synovial (facet) joints of vertebrae -longitudinal deep (epaxial) muscles of back -overlying skin |
|
|
Anterior Ramus
|
-course around body wall to supply anterolateral skin, hypaxial muscles of neck and trunk, including skin, muscles, joints of the limbs
-anterior rami merge and interchance of fibers with adjacent anterior rami, forming plexuses. Contribute to peripheral nerves which have multisegmental distributions -but simple spinal nerves (T2-L1) remain separate (unisgemental) and can usually be traced by dissection to the muscles and skin that each innervates. |
|
|
Vertebral column
|
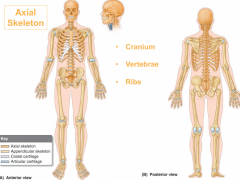
-bodies of all vertebrates build on central axis
-a series of bones connected by joints and ligaments -derived from somatic mesoderm (sclerotomes) -primary component of the axial skeleton (cranium, vertebrae, ribs) |
|
|
Functions of vertebral column?
|
-absorbs shock and transmits weight of body
-provides partly rigid and flexible core axis for body, pivot for head -enables stature and posture (maintaining head and truck erect) -transmit body weight to lower limbs -provides base for locomotion, manipulation -protection the spinal cord, nerve roots |
|
|
Embryonic vertebral column
|
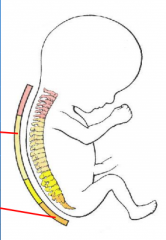
-"C" like curvature
-primary curvatures (kyphoses) at thoracic and sacral -concave anteriorly -this persists through life |
|
|
Developing/Adult vertebral column
|
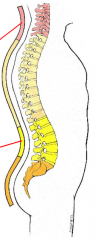
-posterior concave secondary curves (lordoses form) in cervical and lumbar regions.
-cervical develops in infant to attain head control in prone position -lumbar for erect position and walking |
|
|
Hyperkyphosis
|

-excessive thoracic kyphosis (hump-back)
-result of erosion or compression fracture of the anterior part of vertebrae -dowager hump in osteoporosis |
|
|
Hyperlordosis
|

-excessive lumbar and or cervical lordosis
-characterized by an anterior rotation of vertebral column resulting in a rib hump during flexion of trunk |
|
|
Scoliosis
|
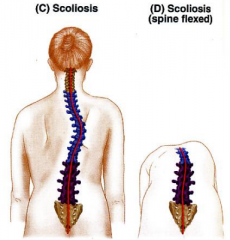
-crooked or curved back
-lateral bending and rotation of vertebral column -may be postural due to posture (reversible); or structural- due to anomalous vertebrae, differential length of the lower extremities |
|
|
Parts of typical vertebrae
|
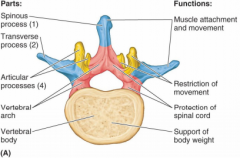
1. vertebral body
2. vertebral arch and associated seven bony processes (arise from vertebral arch) |
|
|
Vertebral body
|
-anterior portion of verebrae
-gives column strength, supports body weight -spongy bone surrounded with think layer of compact bone -held together by intervertebral discs (fibrocartilage) and ligaments -column of bodies and discs creates flexible rod -osteoporosis (loss of bone density)--> crush fractures, excess thoracic kyphosis |
|
|
Vertebral arch
|
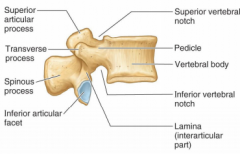
-encase spinal cord
-formed by pedicles (join to body) and lamina (two broad flat plates of bone form posterior part of vertebral foramina) |
|
|
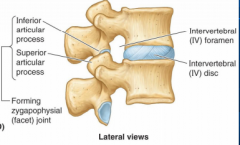
Seven bony processes
|
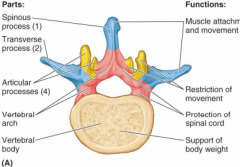
-arise from vertebral arch
-spinous processes (1) and transverse processes (2) provide attachment for muscles, serving as levers to produce movement and for ligaments limit range of motion -articular processes (4)- from zygapophysial (facet) joints with vertebrae above and below |
|
|
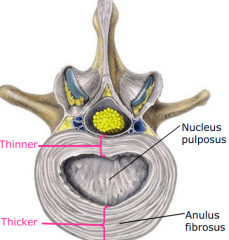
Intervertebral discs
|
-joints of vertebral bodies (IV discs)
-summed together, IV discs account for 25% of height of vertebral column -symphyses-fibrocartilagenous joints uniting two adjacent vertebral bodies -thickness largest in lumbar region -function: 1. movement 2. force dissipation 3. resists displacement -have two basic components: anulus fibrosis and nucleus pulposus |
|
|
anulus firbosis
|
-peripheral lamellae of oblique, dense collagen fibers.
-thinner -site of disc herniations -the superfacial layers are innervated by recurrent meningeal branch of spinal nerve |
|
|
nucleus pulposus
|
-gelatinous
-collagen in semisolid matrix, can imbide fluid -mostly water content -overall height decreases with extended weight-bearing, age |
|
|
zygapophysial (facet) joints
|
-plane type of synovial joint
-thoracic region: facet joints in frontal plane with tilt towards saggital plane. permits rotation, some side bending -lumbar region- flexion, extension. limiting bending and rotation -transition is abrupt. subcervical vertebrae most vulnerable to injury (vertebra T-12) |
|
|
synovial joint
|
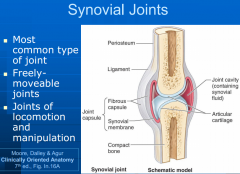
=moveable joints between two or more rigid skeletal components (bone,cartilage)
-articular surfaces covered by articular cartilage within joint cavity containing lubricating synovial fluid, enclosed by joint capsule -joint can be affected by arthritis -facet joints are plane type synovial joints |
|
|
Thoracic region specializations
|
-12 vertebrae, each associated with a pair of ribs
--typical thoracic vertebrae bear two pairs of inferior and superior costal facets on body for articulation with heads of ribs --transverse processes bear transverse costal facets to articulate with tubercle of rub |
|
|
Lumbar region specializations
|
-5 typical vertebrae
-no facets on body, transverse processes -short, stout spinous processes and pedicles -long transverse processes |
|
|
Ligaments of vertebral column
|
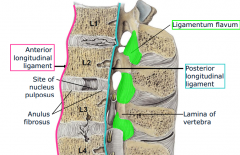
-Anterior longitudnal ligament- resists hyperextension (whiplash)
-posterior longitudinal ligament - resists hyperflexion -ligamentum flavum- yellow, elastic ligament connecting adjacent laminae |
|
|
Vertebral canal and intervertebral (IV) foramina
|
-vertebral foramina consists of canal, spinal cord, roots, coverings.
-IV foramina- lateral passageways where spinal nerves exit *lumbar spinal nerves increase in size from above downward, but intervertebral foramina decrease in caliber *spinal nerves exit superior part of IV foramen. herniation does not affect nerve exiting at same level of disc, but nerve traveling on level below |
|
|
Epaxial muscles
|
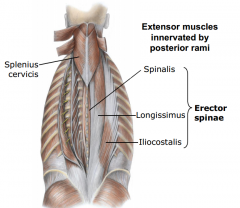
-extensor muscles of back proper (intrinsic muscles of back)
-enveloped by thoracolumbar fascia -originate from and insert on elements of axial skeleton, located posterior to axis -received multi-segmental innervation by posterior rami (large muscles to be contracted to various degrees, specific portions to contract spasmotically) |
|
|
Epaxial muscle layers
|
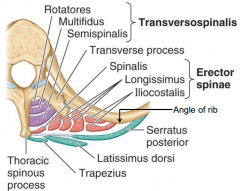
1. superficial layer: splenius muscles
2. intermediate layer: erector spinae muscles -large muscle mass between spinous process and angles of ribs. a. lateral column-iliocostalis b. intermediate column-longissimus c. medial column- spinalis 3. deep layer-transversospinal muscle groups -deep to the erector spinae -arise from transverse process, attach cranially to spinous process -semispinalis, multifidus, rotatores posture control muscles- contain high density of neuromuscular spindles (and organs for proprioception-sense of movement and position) |
|
|
Spinal cord function
|
-major reflex center
-impulse conduction pathway between body and brain |
|
|
Spinal cord external anatomy
|

-CNS extends between level of atlas C1 to L1, L2
1. cervical enlargement (C4-T1)-associated with brachial plexus (innervation of upper limb) 2, lumbosacral enlargement (T11-L1)-associated with lumbar and sacral plexuses (innervation of lower limb) 3. conus medullaris - inferior to lumbar enlargement, associated with lumbar and sacral plexuses (innervations of lower limb) 4. filum terminale- continuation of pia mater, extending as a slender anchoring filament from the tip of the conus medullaris |
|
|
Spinal cord in adult vs at 12 weeks gestation
|

-in adult- spinal cord ends at ~L2 vertebral level
|
|
|
Cauda equina
|
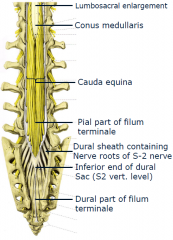
composed of dorsal and ventral roots of lower lumbar and sacral spinal nerves inferior to termination of spinal cord
-located in lumbar cistern of subarachnoid space |
|
|
Where is CSF?
|
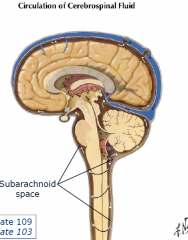
Circulates in the subarachnoid space
|
|
|
3 Layers of Connective Tissue covering spinal cord, vertebral column
|
-spinal meninges
1. dura mater (outermost, forms dural sac) 2. arachnoid mater 3. pia mater |
|
|
Dura mater
|
-outermost, most substantial CT covering
-tapering lateral extensions, the dural root sheaths (sleeves) surround terminal parts of uniting posterior and anterior spinal nerve roots -epidural space is superficial to sac |
|
|
spinal arachnoid mater
|
-middle layer
-delicate, avascular membrane -dura-arachnoid space lies between dura and arachnoid |
|
|
spinal pia mater
|
-innermost, mostly transparent layer
-thickened, visible -extends laterally between roots on each side as continuous denticulate ligaments -arachnoid and pia mater are parietal and visceral layers of one continuous membrane, the leptomeninges -space enclosed is the subarachnoid space= CSF |
|
|
CSF
|
-straw colored transparent fluid where CNS is suspended
-actively secreted in ventricles of brain -protection of CNS, nutrition of surface cells |
|
|
Lumbar puncture
|
-used to sample CSF
-patient lying on side with trunk flexed -at L3-L4 or L4-L5 vertebral level Punctures through 1. skin 2. fat 3. supraspinous ligament 4. interspinous ligament 5. ligamentum flavum (pop) 6. dura mater (second pop) 7. arachnoid mater 8. subarachnoid space |
|
|
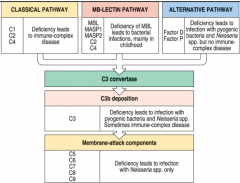
C1 deficiency
|
-specific gene mutation
-defect in classical pathway -immune complex disease |
|
|
mannose-binding lectin deficiency
|
-lectin pathway
-susepcitble to bacteria |
|
|
C2 or C4 deficiency
|
-classical/lectin pathway defect
-susceptible to bacteria and immune complex disease |
|
|
D or P deficiency
|
-alternate pathway defect
-suseptible to pyogenic bacteria, Neissaria |
|
|
C3 deficiency
|
-all pathways defect
-trouble with pyogenic bacteria, Neisseria, immune complex disease |
|
|
C5-C9 deficiency
|
-MAC complex formation defect
-susceptible to Neisseria |
|
|
Paroxysmal nocturnal hemoglobinuria
|
-abnormality in GPI synthesis
-defect in DAF, CD59, HRF expression by RBC -red blood cell destruction |
|
|
hereditary angioneurotic edema
|
-abnormality of C1 inhibitor
-no inhibition of C1r, C1s, factor XII, kallikrein -leads to intestinal, skin, airway swelling |
|
|
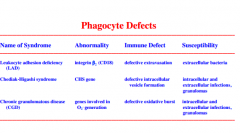
Leukocyte adhesion deficiency (LAD)
|
-defect in integrin B2 (CD18)
-defective extravasation, phagocytes cannot enter tissues -leads to extracellular bacteria -no profound defects in T cell extravasation |
|
|
Chediak-Higashi syndrome
|
-CHS gene
-defective intracellular vesicle formation -so phagocytes have impaired intracellular killing -susceptible to intracellular and extracellular infections, granulomas -other abnormalities like partial albinism, abnormal platelet function |
|
|
Chronic granulomatous disease (CGD)
|
-defect in genes involved in oxygen radical generation
-defective oxidative burst -leads to intracellular and extracellular infections, granulomas |
|
|
NK cell defect
|
-abnormality unknown
-no NK cells -herpes virus -many herpes viruses downregulate MHC class I expression |
|
|
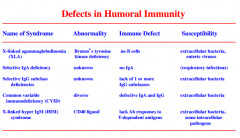
X-linked agammaglobulinemia
|
-Bruton's tyrosine kinase deficiency
-few B cells, these B cells have activation defects -leads to extracellular bacteria, enteric viruses |
|
|
Selective IgA deficiency
|
-unknown abnormality
-most common inherited form of Ig deficiency (1/500) -no IgA -respiratory infections |
|
|
Selective IgG subclass deficiencies
|
-unknown abnormality
-lack of 1 or more IgG subclasses. but normal IgG total. -enhance suseptibility to pyogenic infections -extracellular bacteria |
|
|
Common variable immunodeficiency
|
-diverse abnormalities
-defective IgA and IgG -extracellular bacteria |
|
|
X-linked hyper IgM (HIM) syndrome
|
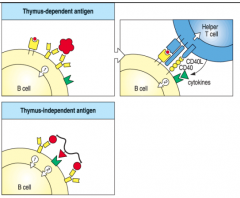
-CD40 ligand abnormality
-defective production of IgG and IgA, enhanced IgM production -lack Ab responses to T-dependent antigens -lack germinal centers -extracellular bacteria, some intracellular pathogens |
|
|
X-linked SCID
|

-yc chain deficiency
-no T cells, defective B cells -general susceptibility |
|
|
JAK3 deficiency
|
-JAK3 mutation, defective yc signalling
-no T cells, defective B cells -general suseptibility |
|
|
ADA deficiency
|
-adenosine deaminase deficiency
-accumulation of nucleotide metabolites that are toxic to developing T cells -no T cells, reduced B cells -general susceptibility |
|
|
PNP deficiency
|
-purine nucleotide phosphorylase deficiency
-accumulation of nucleotide metabolites that are toxic to developing T cells -no T cells, reduced B cells -general susceptibility |
|
|
RAG deficiency/ Omenn syndrome
|
-RAG-1 or RAG-2 defects
-Defects in VDJ recombination -Omenn-residual RAG activity, abnormally activated T cells -no or reduced B and T cells -general susceptibility |
|
|
DiGeorge syndrome
|
-deletion on chr. 22q11.2
-small thymus/few T cells -general susceptibility -also defective development of parathyroid glands, other structure developing from third and fourth pharyngeal pouches during fetal life |
|
|
Bare lymphocyte syndrome
|
-abnormality in MHC class II expression (TF mutated)
-few or no CD4 T cells -general susceptibility |
|
|
APS-1/APECED
|
-abnormality in AIRE (there is no thymic expression of peripheral self-antigens, so now no negative selection of autoreactive T cells)
-autoreactive T cells -leads to autoimmunity -endocrine problems |
|
|
IPEX
|
-abnormality in Foxp3, which is critically important for the intrathymic development of Tregs
-no Tregs -autoimmunity/allergy |
|
|
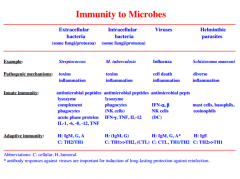
Immune responses against microbes
|
|
|
|
Discuss how a patient's history of infections can be used to identify the type of host defense defect
|
1. recurrent infection with pyogenic bacteria- defects in antibodies, complement, phagocyte function
2. recurrent infection with intracellular pathogens in addition to pygoenic bacteria suggests T cell defects (or combined B/T) |
|
|
The immune system protects against four classes of pathogens
|
-extracellular bacteria, parasites, fungi
-intracellular bacteria, parasites -viruses (intracellular) -parasitic worms (extracellular) |
|
|
Immunological tests of human immune competetence
|

|
|
|
What are the different categories of congenital immunodeficiencies?
|
-Defects in innate immunity (complement, phagocytes, NK cells)
- immunodeficiences that are primarily caused by defective humoral immunity - immunodeficiences that are due to defective cell-mediated and humoral immune responses |
|
|
Complement functions
|
1. punch holes in microbial cell walls, cellular membranes (MAC complex)
2. induce inflammation by inducing the release of histamine and by attracting and activating neutrophils 3. to prepare microbes for phagocytosis (opsonization) 4. to remove circulating immune complexes |
|
|
Complement deficiencies
|
|
|
|
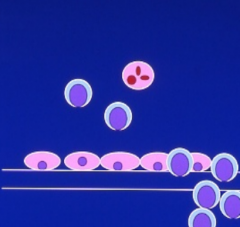
Extravasation
|

When phagocytes (neutrophils and monocytes/macrophages) reach crime scene by emigrating from blood vessels
a. P, E-selectins on inflamed endothelium interact with sugar ligands (sialyl-Lewis) on phagocytes b. chemoattractants (IL-8) bind with receptors on phagocytes c. activated phagocyte integrins (LFA-1) bind with Ig superfamily ICAM on endothelium |
|
|
Phagocyte defects
|
|
|
|
Defects in Humoral Immunity
|
|
|
|
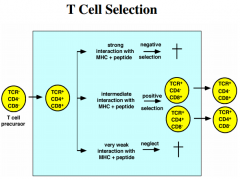
T Cell selection (review)
|
|
|
|
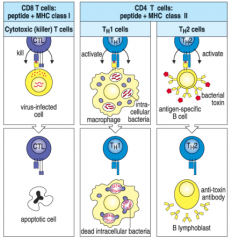
CD4 and CD8 T cells
|
|
|
|
Therapeutic approaches for congenital immunodeficiencies
|
1. Enzyme replacement therapy- treat complement inhibitor deficiency (frozen plasma, recombinant proteins), also treatment of ADA, PNP deficiencies (RBC source of enzyme)
2. Passive immunizations- IVIG (intravenous immune globulin) for XLA. treat in defects of antibody-mediated immunity 3. bone marrow transplantation- for SCID and LAD. complications with host-versus graft, graft vs host disease 4. Gene therapy- obtain patient's stem cells, insert normal copy of defective gene, return cells to patient. but under fire because of deaths |
|
|
bacteremia
|
presence of viable bacteria in the blood
|
|
|
opportunistic infections
|
infections due to an agent that does not harm a healthy host but takes advantage of an unhealthy one (e.g. in inherited or acquired immunodeficiency). Important examples of opportunistic pathogens are Toxoplasma, Mycobacterium avium intracellulare, Pneumocystis carinii, Candida
|
|
|
pyogenic bacteria
|
-bacteria that produce pus (bacterial cell derbis and dead neutrophils) at site of infection
-have large capsules that are difficult for phagocytes to ingest. Important examples are Strept pneumoniae, Staph aureus, H. influenza, Pseudomnas aeruginosa |
|
|
septisemia
|
blood poisoning associated with persistence of pathogenic organisms or their toxins in the blood
|
|
|
Transplantation and transfusion
|
-process of taking cells, tissues, or organs (the graft) from one individual and placing them into the same (an autograft) or a different individual.
-transfusion is a transplantation of circulating blood cells and/or plasma from one individual to another |
|
|
ABO antigens
|
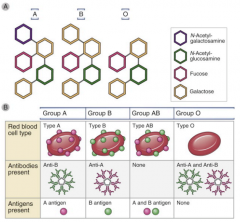
-antigens represent carbohydrate modifications on proteins, or lipids. Modifications are made by the products of A or/and B alleles, whereas the product of the O allele lacks enzymatic activity.
-Antibodies IgM made by B1 cells, marginal zone B cells (no class switch recomb). -T cell independent antibody response -Activation of complement system- uptake by phagocytes and lysis (type II hypersensitivity). hemoglobin liberation, massive cytokine release |
|
|
Rhesus antigens
|
-protein on RBC
-Rh-negative cannot tolerate Rh antigen -T-cell dependent, B cells can induce class-switch to generate IgG. IgG can enter fetus, induce lysis of fetal RBC |
|
|
Hemolytic reaction during pregnancy
|
--Development of erythroblastosis fetalis: generation of anti-Rh IgG antibodies when Rh+ fetus develops in Rh- mother.
-first pregnancy fine, but IgG plasma cells made. -Treatment with antibodies (Rhogam) against Rh antigens at time of delivery can prevent condition (prevent B-cell activation, memory cell formation) |
|
|
Determination of blood group types
|

Use agglutination assay with anti-A, anti-B, anti-Rh antibodies
|
|
|
Pathologic pattern of tissue graft rejection
|
|
|
|
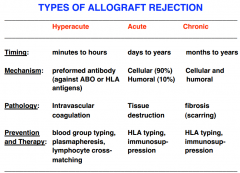
Hyperacute rejection
|
-occur in minutes, hours
-rapid thrombotic occlusion of graft vasculature (intravascular coagulation) -caused by natural antibodies against blood group antigens, antibodies against HLA molecules. -can be prevented by matching of blood group antigens, testing recipients for antibodies against the graft. also plasmapheresis |
|
|
Acute rejection
|
-start after several days. episodes can occur for several years
-predominantly caused by effector mechanisms of alloreactive T lymphocytes --CD8 killing of grafted tissue, CD4 release of cytokines. also some humoral response can contribute -can be prevented by MHC matching and immunosupressants |
|
|
What is the molecular basis for the recognition of foreign MHC molecules by T lymphocytes?
|
1. MHC molecules and antigen processing- MHC locus most polymorphic region in geonme. Individuals generally express different MHC molecules in co-dominant way. self proteins can be degraded and expressed at cell surface on MHC
2. TCR interacts with foregin peptide antigen and residues of a-helicies of MHC molecule. This is basis for self-MHC restriction. Positive selection- T cells recognize self MHC, recognize foreign antigens only *alloreactivity reflects cross-reactivity of T cell receptors normally specific for self MHC + foreign peptide with foreign MHC + self peptide. Thus in some cases, self MHC + foreign peptide resembles foreign MHC + self peptide, resulting in molecular mimicry |
|
|
Chronic rejection
|
-start after several months, can last for many years
-chronic rejection: chronic inflammation, repair, firosis of normal organ structures. -pathologic mechanisms poorly understood. -cellular and humoral. immunosupressants and anti-inflammatory agents used to treat chronic rejection |
|
|
Strategies for prevention and treatment of graft rejection
|
1. reduce immunogenicity of the graft by tissue matching
2. immunosupression with drugs 3. immunosuppression with antibodies |
|
|
Prevention of allograft rejection by cell and tissue typing
|
-match ABO groups to minimize hyperacute
-match allelic differences of MHC class I and II loci (HLA) -use HLA typing (antisera recognizing specific HLA alleles or DNA sequencing following PCR) -HLA matching promotes acceptance of kidney grafts, bone marrow grafts, but not critical for liver or cornea transplantation |
|
|
Treatment of allograft rejection by immunosupression
|
major approach
1. inhibit inflammation with corticosteroids (prednisone)-pharma derivatives of GC family of steroid hormones. they inhibit cytokine production, inhibit adhesion molecule expression 2. kill with cytotoxic drugs (mycophenolate mofetil, azathioprine)- interfere with DNA synthesis 3. inhibition of T lymphocytes with clcyosporin A, tacrolimus, rapamycin (immunosupressive, interfere with T cell signalling). bind with immunophilins, complexes interfere with calcineurin, which is involved in TCR T-cell signalling. Inhibit cytokine IL-2, T-cell activation and proliferation. Rapamycin- inhibits IL-2 binding to receptor. |
|
|
Inhibition of allograft rejection with monoclonal antibodies
|
-treatment of recipients with T-cell specific antibodies to remove T lymphocytes has been used successfully in clincal practice.
-blocking antibodies against IL-2 receptor can inhibit T cell activation |
|
|
Appreciate that reactions during hematopoietic stem cell transplantation may involve recipient and donor immune components
|
-HSC transplants most commonly performed for hematopoietic malignancies
-T cells from recipient may react with donor cells, causing graft loss -grafted cells from donor may contain small number of lymphocytes that attack recipient tissues. GVHD disease. -stem cell grafts for treatment of hematopoietic malifnancies, limited GVHD can be beneficial in destroying residue |
|
|
Normal joint
|
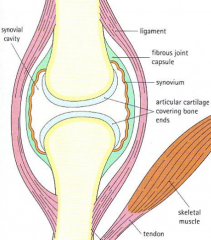
Joint consists of:
articular cartilage articular capsule Articular capsule: Fibrous capsule Synovial membrane Synovial fluid --hyaluronic acid |
|
|
3 types of joints
|
fibrous, cartilaginous, synovial
|
|
|
synovial joints
|
-allow for low friction movement between opposing bones. the articular cartilage is elastic, joint is filled with fluid
-consists of (1) articular cartilage (covers ends of bone) (2) articular capsule consisting of fibrous capsule surrounding joint and synovial membrane lining cavity (3) joint cavity filled with synovial fluid. join reinforced by ligaments |
|
|
synovial fluid
|
-formed by ultrafiltration of blood into which hyaluronic acid is secreted. Hyaluronic acid gives synovial fluid high viscosity to act as lubricant
|
|
|
Rheumatoid arthritis- introduction
|
-chronic systemic inflammatory disease primarily involving joints leading to profound deformity, disability, and premature mortality.
-affect 1% of Americans -3:1 female predominance, older individuals |
|
|
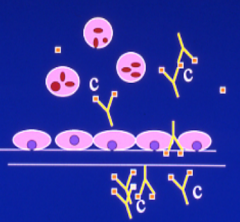
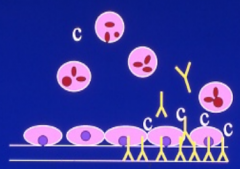
Rheumatoid arthritis- Pathogenesis
|
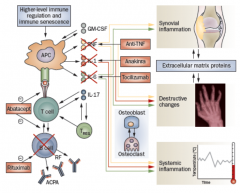
![1. Immune complex mediated inflammation [plasma cells in synovium produce IgM, IgG (Rheumatoid factors) against Fc portion of IgG]. These complexes formed activate complement, trigger release of PMNs, macrophages with inflammation
2. Pannus for...](https://images.cram.com/images/upload-flashcards/71/24/42/2712442_m.png)
1. Immune complex mediated inflammation [plasma cells in synovium produce IgM, IgG (Rheumatoid factors) against Fc portion of IgG]. These complexes formed activate complement, trigger release of PMNs, macrophages with inflammation
2. Pannus formation- proliferating hyperplastic "villus like" projections of synovial tissue which spread over articular cartilage. [pannus destroys cartilage by interfering with synovial fluid flow into cartilage (no O2, glucose for chondrocytes), and delivers degradative enzymes like collagenase and elastase to surface of cartilage)] -*CD4 T cells trigger pannus formation, activate synovial lining cells on surface of pannus to degrade cartilage 3. Inflammation + pannus formation cause destruction of cartilage, weakened joint support with eventual deformity and ankylosis (fusion of joint) |
|
|
Rheumatoid arthritis- Clinical expression of disease
|
1. constitutional symptoms: fever, malaise, weight loss (cytokine IL-1, TNF)
2. arthritis: start in small joints of hands/feet, progresses in centripetal and symmetric fashion. Swelling erythema, pain, limited mobility of affected joints. Late sequelae: ankylosis (fusion of joint) 3. extra-articular disease: these pts have circulating IgM rheumatoid factors --20-25% patients have rheumatoid nodules- in soft tissue adjacent to joints (central fibrinoid necrosis surrounded by rim of palisading macrophages) --pleural/pericardial disease --vasculitis- occulsion of small arteries producing gangrene to systemic acute vasculitis. vessel wall deposition of immune complexes causing this vasculitis |
|
|
Rheumatoid arthritis- Laboratory
|
-85% patients of circulating IgM rheumatoid factors
-Antibodies to citrulline-modified peptides [CCP] |
|
|
Rheumatoid arthritis- Course/Prognosis
|
-Sizable minority of patients progress to total disability
|
|
|
Systemic Lupus Erythematosus (SLE)- Introduction
|
-multisystem inflammatory disease characterized by the production of multiple autoantibodies, particularly antinuclear antibodies
-may affect almost any organ in the human body |
|
|
SLE- epidemiology
|
20-50/ 100,000
Female > Male 9:1 Age of onset (65% between 16 and 55) |
|
|
SLE-pathogenesis
|
-disordered immune regulation with production of autoantibodies to host of nuclear, cytoplasmic, and membrane antigens
-IMMUNOLOGIC FACTOR: failure of regulatory mechanisms that sustain self-tolerance. -Antinuclear antibodies (ANA) made to antigens from active sites on molecules involved in essential cellular functions 1)Ab to DNA, 2)Ab to histones, 3) Ab to non-histone protein bound to RNA, 4) Ab to nucleolar antigens |
|
|
SLE- Immunologic Abnormalities
|
-abnormal processing of nuclear and other self-antigens by APCs
-formation of peptide-MHC complexes -clonal expansion of CD4+ auto reactive T cells & auto reactive B-cells with production of auto antibodies -ANAs are complement fixing of IgG subclass, form immune complexes- type III hypersensitivity |
|
|
SLE- Clinical features
|
1. Constitutional-fever without infection, weight loss, fatigue
2. Arthritis 3. Serositis- pleuritis and pericarditis- linings over heart and lungs 4. Dermatitis (butterfly rash to alopecia to vasculitis of dermal vessels)- dengereation of basal layer of epidermis, perivascular mononuclear infiltrates in dermis. Deposition of IgG and C3, complement at dermal-epidermal junction 5. Renal disease 6. CNS-psychosis, seizure disorder. occlusion of small vessels 7. cardiac disease-pericarditis, valvular abnormalities 8. infection 9. hypercoagulability- antiphospholipid antibody syndrome (APS)- autoantibodies against phospholipids, plasma proteins bound to anionic phospholipids. Ab: (lupus anticoagulant, anticardiolipin) |
|
|
SLE- laboratory
|
-99% will have positive ANA
-Highly-specific is anti-dsDNA -More highly specific but only present in 30% patients is Smith antigen |
|
|
Antiphospholipid antibody syndrome
|
APS is caused by auto-antibodies against phospholipids, plasma proteins bound to anionic phospholipids
-venous and arterial thromboses, recurrent fetal losses, neurological events, thrombocytopenia -lupus anticoagulant, anticardiolipin antibody |
|
|
Drug-induced lupus
|
-hydralazine, procainamide, isoniazid
-slow acetylators develop ANAs, symptoms sooner. Acetylation is metabolism of drugs in liver -Resolution of symptoms and ANA when drug is withdrawn |
|
|
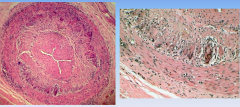
Vasculitis
|
-inflammation that causes structural damage to a vessel wall
-can be primary or secondary (RA, SLE, heaptitis, neoplasm, secondary to drug reaction) -vascular inflammatory injury |
|
|
Vasculitis- classification
|
-Most important consideration is caliber/size of vessel
(large-aorta, largest branches) (medium-renal arteries, hepatic artery) (small-arterial radicals that connect with arterioles) -organ involves, type of inflammation, lab findings, clinical features |
|
|
Vasculitis-common mechanisms
|
1. direct infection by organism (bacteria-Nesiserria, rickettsia, spirochetes, fungi, viruses)
2. immune mediated- complex mediated, direct antibody attack, anti-neutrophil cytoplasmic antibody, T cell mediated |
|
|
Vasculitis- Immune complex (IC) mediated
|
-deposition of circulating IC in vessel- complement activated, PMNs, monos circulate.
-example is serum sickness -IF: granular pattern |
|
|
Vasculitis- direct antibody attack
|
-autoantibodies directed against consitutuents of vessel walls can mediate vascular injury
-in situ immune complex formation, activate humoral and cellular mediators of inflammation. -example is Goodpasture's syndrome (against basement membrane). -IF is linear pattern |
|
|
Vasculitis- ANCA
|
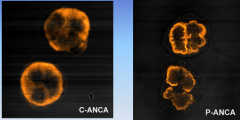
-antineutrophil cytoplasmic antibodies (ANCA)
-autoantibodies against enzymes and antigens found in cytoplasma of PMNs. -IF: c-ANCA in cytoplasm for proteinase-3 (more in Wegeners) --p-ANCA for perinuclear staining, myeloperoxidase -example is Wegener's granulomatosis (15% in SLE) |
|
|
Vasculitis- cell-mediated
|
-T-cell driven
-T cells adhere to vascular endothelium , penetrate intima and musclaris, inducing mononuclear cell infiltrate -example is acute rejection in transplant setting |
|
|
Vasculitis- laboratory tests
|
1. Serologic
- nonspecific (acute phase reactants, erythrocyte sedimentation rate). ESR- acute phase reactants- more of these will induce longer fall of column of RBCs in given length of time. (incr fibrinogen, c-reactive protein- less negative charge) -more specific (specific autoantibodies) 2. Tissue biopsy -light microscopy -immunofloresnce (IF) |
|
|
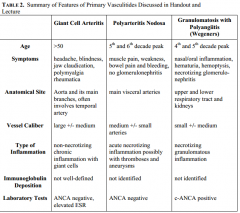
Giant cell (temporal arteritis)
|
-Large vessel vasculitis: aorta and its branches (extracranial branches of carotid, arteries in head)
-most often temporal artery -granulomatous inflammation -headaches, blindness, weight loss, fever -ANCA negative, steroid treatment |
|
|
Polyarteritis nodosa (PAN)
|
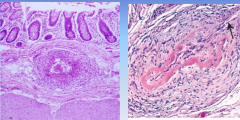
-50-60s y/o
-necrotizing inflammation of medium-sized and small arteries. visceral arteries -at branch points, can form aneurysms detected by angiography -bowel pain, bleeding. muscle pain, weakness, chest pain. |
|
|
Granulomatosis with polyangiitis (wegener's)
|
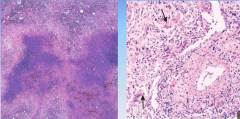
-small and medium sized vessels
-affects upper, lower respiratory tract and kidneys, can involve cutaneous vessels -necrotizing granulomatous inflammation -c-ANCA -nasal, oral inflammation, hemoptysis, hematuria, palpable purpura. -Treat with cytoxan |
|
|
Primary vasculititides summary
|
|
|
|
Distinguish inflammation associated with infectious diseases from disorders characterized by inflammatory processes
|

-gout would see uric acid crystals
-infectious process will see bacteria? pathogens? |
|
|
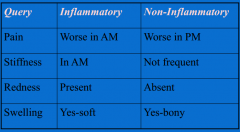
Gout
|
-classically an acute, hot joint
-first MTP involved at some point -not present in pre-menopausal females -diagnostic arthrocentesis -treat with NSAIDs, steroids, colchicine (first few hours, poorly tolerated) , IL-1inhibitor -agents to lower uric acid (allopurinol, colchicine) |
|
|
Lupus drug therapy
|
-hydroxychloroquine- prophylactic for malaria, changes mysosomal pH, interferes for antigen presentation, processing. very safe drug beneficial for skin rash, etc
-glucocorticoids- complications, each bruising, high dosing has side effects -NSAIDs- serositis-pleuritic pain, arthritis -for serious lupus neprhtiis, CNS lupus: cyclophosphamide, and mycophenylate mofetil |
|
|
Sensitivity vs Specificity
|
ANA- positive in 99% of patients with lupus. 1/100 normal individuals will be positive. prevalence of disease is 1/2000. have 20 positive tests to have one person with lupus. increase to 1/3 if include arthritis
|
|
|
Osteoarthritis
|
-wear and tear only part of story
-generalized osteoarthritis has genetic links -inflammatory component is present in many cases -most prevalent form of arthritis -Diagnostic- X-ray. bony changes usually include marginal osteophytes -Treatment: weight loss, exercise, aqua therapy. acetaminophen/cautious NSAIDs, Hyalan (synvisc) |
|
|
Inflammatory or non-inflammatory problem?
|
|
|
|
Rheumatoid arthritis
|
-most common serious autoimmune disease
-1% in population in US -affects middle age people during productive phases of life. accelerates overall mortality |
|
|
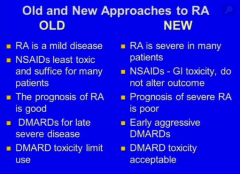
Management of rheumatic diseases
|
1. simple analgesics
2. NSAIDs 3. Corticosteroids 4. DMARDs goals: relieve pain, maintain and restore function, maintain and restore strength, prevent progression Treat at early stage! Severe RA is associated with decreased survival |
|
|
Old and new approaches to RA
|
|
|
|
ACR20
|
-20% in tender-joint count or swollen-joint count would be in the criteria of success
"american college of rheumatology" -achieved in half of RA patients with LEFLUNOMIDE, METHOTREXATE |
|
|
Methotrexate in RA
|
mechanism of action- inhibits dihydrofolate reductase, increases adenosine
clinical use is oral, weekly, low dose minor toxicities, very well tolerated follow CBC, liver function monitoring. dont give to alcoholics |
|
|
Hydroxychloroquine
|
-milder disease, slow onset, combination therapy
- |
|
|
Sulfasalazine
|
-alternate to methotrexate, leflunomide
-used RA, AS, psoriatic arthritis low efficacy, low toxicity |
|
|
Leflunomide
|
-inhibits pyrimidine syntehsis.
-efficacy -teratogenic -half life is 2 weeks -less hepatotoxicity than methotrexate, although black box warning |
|
|
anti-TNF
|
-serious RA (doesnt respond to other drugs)
-Infliximab IV, adalimumab sc, all anti-tnf antibodies -Etanercept- soluble TNF-receptor fused to Ig tail -anti-TNF also used in inflammatory bowel disease -with introduction of anti-TNF, a lot more ACR50 -adverse effects: infections, injection reactions-antinuclear antibodies/lupus (change Th1 to Th2) response, demyelination, malignancy, cardia, hep B reactivation |
|
|
IL-1 inhibition
|
-Anakinra (IL-1Ra)
-canakinumab- monoclonal antibody with longer half life. treat some gout too? -gene therapy -IL-1 trap- high affinity blockers of cytokine action |
|
|
IL-6 inhibition
|
Tocilizumab- humaized anti-human IL-6 receptor antibody of IgG1 subclass.. inhibits binding of native cytokine to its receptor and interfering with cytokine's effects
|
|
|
Costimulation blockade
|
-eliminate second signal
-CD28/CTLA-4 (CTLA-4 downregulates immune system) can bind to B7-1 or B7-2 -Abataceppt comprises CTLA-4 and Fc portion of IgG1. precents CD28 from binding to B7 |
|
|
B-cell depletion
|
-Rituximab is B-cell depleting monoclonal anti-CD20 antibody.
-uses mechanisms of Fc receptor gamma-mediated antibody-dependent cytotoxicity, antibody-dependent complement-mediated cell lysis, growth arrest, B-cell apoptosis. But plasma cells levels do not change (CD-20 only in B-cell devleopment) |
|
|
Summary of biologics for treatment of rheumatic diseases
|
|
|
|
Combination therapy for RA
|
Methotrexate + sulfasalazine + hydroxychlorquine
methotrexate + TNF antagonists Methotrexate + other biologics do not combine biologicals |
|
|
Staphylococcus introduction
|
-most virulent is S. aureus
-gram positive, pyogenic- form abscesses, septic shock, wound infections, endocarditis, skin and bone infections, toxic shock syndrome, food poisioning -MRSA strains, ca and ha-acquired |
|
|
Staph Microbiology
|
S. epidermidis, S. saprophyticus (urinary tract in young women) are coagulase-negative. they can produce biofilm. infection of retained prostehetic.
Only S, aureus makes coagulase- clots plasma. clumping will occur. Staphylococci are aerobic, facultatively anaerobic, non-motile, gram positive cocci. do not form spores. primary reservoir is humans. in nares of 30% of healthy people. on inanimate objects as well |
|
|
Staph Pathogenesis-colonization
|
Colonization- MSCRAMMs- microbial surface components recognizing adhesive matrix molecules.
1. fibronectin-binding proteins (FnbpA/B) attack to exposed fibronectin in wounds, enable bacteria to invade deeper tissues 2. CNAs- collage-N-terminal adhesin- bind to collagen, facilitate arthritis, endocarditis, osteomyelitis thru CT, bones, joints 3. coagulase- converts fibrinogen to fibrin. clot is the excellent hiding place for bacteria because neutrophils cannot penetrate 4. catalase- converts H2O2 to water, countering ability of neutrophils to kill bacteria |
|
|
Staph pathogenesis- damage
|
1. peptidoglycan of gram + bacteria- interact with TLR2, lead to sepsis
2. teichoic acid helps adherance to mucosal cells, activates complement leading to septic shock 3. hemolysins, panton-valentine leukocidin (PVL)- pore forming toxin. necrosis, community acquired MRSA 4. proteases, enzymes like proteases, lipases, elastases to invade, destroy host tissues. once immune system and coagulation pathways activated, septic shock. 5. quorum sensing-hold back until population reaches critical mass. cell-to-cell communication- small autoinducer molecules. biofilm development. |
|
|
Staph pathogenesis- avoiding immune system
|
1. biofilm-slime that adheres to host, prosthetic surfaces, can hide in this slime. Impossible to cure infection without surgically removing device and slime
2. small colony variants can hide inside cells protected from antibiotics, host defenses. they survive inside epithelial and endothelial cells. can revert to more virulent wildtype later 3. anti-phagocytic microcapsule. promotes abscess formation. Protein A binds to Fc part of Ig. Leukocidin destroys leuckocytes with pores |
|
|
Staph clinical characteristics
|
-pimples, boils on skin. localized host response is inflammation, elevated temperature, swelling. necrosis of tissue. fibrin clot may form, abscess.
-furnucles, impetigo possible -can spread to bone via hematogenously. -septicemia (bactermia with fever) *Toxin related disease: 1. Staphylococcal scaled skin syndrome (SSSS)-exfoliative toxins A and B. extensive sloughing of skin. 2. Toxic shock syndrome-associated with highly absorbent tampons. Toxins involved included toxic shock syndrome toxin-1, staph entertoxins- super antigens. Massive cytokine release. fever, hypotension, rash, dysfunction in organ systems 3. Staph food poisoning-ingestion of enterotoxins. Highly heat resistant prepared via infected food handler. nausea and vomiting |
|
|
Staph- MRSA
|
-resistant to methicillin and other anti-staphylococcal penicillins
-MRSA has PBP-2a that allows organism to grow, divide in presence of methicillin and beta-lactam antibiotics |
|
|
Staph- MRSA Epidemiology
|
-hospital-acquired MRSA associated with severe, invasive disease, including skin and soft tissue infection, bloodstream infection, pneumonia.
-leading cause of surgical site infections -risk factors include antibiotic use, prolonged hospitalization, intensive care, hemodialysis, mrsa colonization, proximity to others with mrsa colonization and infection |
|
|
Staph- treatment
|
-MSSA is treated with anti-staphylococcal penicillin such as methicillin (nafcillin)
-treat MRSA with vancomycin, daptomycin -oral agents include dicloxacillin (for MSSA), sulfa drugs, doxycycline, or minocycline (MSSA or MRSA) |
|
|
Staph-prevention
|
-practice hand hygiene
-no vaccine available that stimulates active immunity against staphylococcal infections in humans |
|
|
Streptococcus- microbiology
|
-gram +, non-motile, non-spore forming cocci. catalase NEGATIVE, aerotolerant anaerobe (facultatively anaerboic), requires enriched medium containing blood to grow
- |
|
|
Streptococcus-classification
|
Based on hemolytic reactions:
1. beta-hemolysis- complete lysis of RBC. Group A (S. pyogenes), Group B (S. agalactiae) 2. Alpha-hemolysis- partial or green hemolysis-reduction of red cell hemoglobin. (S. pneumoniae) 3. Nonhemolytic, gamma hemolytic- oral strep and enterococci non hemolytic Lancefield classification: Serotype identification of cell wall components. Most infection causing are in Group A. S. pneumoniae (penumococcus) lacks group specific antigen |
|
|
Group A Strep
|
-Streptococcus pyogenes
-capsule composed of hyaluronic acid and beta-hemolysis |
|
|
Group A Strep- Clinical Illness
|
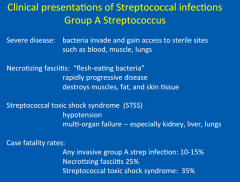
asymptomatic colonization
-present on skin, oropharynx of healthy people. 5-15% harbor bacteria in respiratory tracts mild illness -pharyngitis commonly called strep throat, impetigo infection of superficial layers of skin Also severe disease -bacteria enter blood, muscle, lungs- necrotizing fasciitis, strep toxic shock syndrome, particularly severe forms of group A strep invasive disease. Necrotizing fasciitis--rapidly progressive disease whcih destroys muscles, fat, skin tissue. Streptococcal toxic shock syndrome (STSS) rsults in hypotension, multiorgan failure -Scarlet fever cellulitis- infection of deep layers of skins-Erysipelas post-infectious: rheumatic fever (antibodies attack cardiac tissue, joints), acute glomerulonephritis |
|
|
Group A Strep- pathogenesis
|
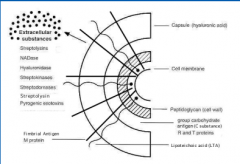
1. Fimbriae- attach to epithelial cells of pharynx or skin. Protrude from cell surface into hyaluronic acid capsule. This is composed of lipoteichoic acid and M proteins
2. M protein is key streptococcal virulence factor-adherence and colonization. 3. capsule inhibits phagocytosis, prevents organism from being recognized by immune system 4. pyrogenic exotoxin- produced by some strep, principal role in triggering STSS, implicated in cause scarlet fever. |
|
|
Group A Strep- transmission
|
-transmitted from infected persons (direct contact with oral and nasopharyngeal secretions, also by contact with infected wounds or other skin lesions)
-complete course of antibiotics! |
|
|
Group A Strep- epidemiology
|
-mild streptococcal infections (strep throat, impetigo)- several million cases in US annually
-invasive group A (STSS, necrotizing)- 1000-1800 deaths -risk groups: Immunocomproised people, elderly, chronic illnesses, alcohol and IV drug users -healthy people can get disease too, but less common |
|
|
Group A Strep- treatment
|
-penicillin. also to erythromycin, clindamycin.
-invasive: penicillin + clindamycin (ribosomally-active antibiotic which may decrease protein synthesis). -necrotizing: early and aggressive surgery |
|
|
Group B Strep
|
-colonize lower GI, vagina. 20-30% prevalence in population
-leading cause of pneumonia, sepsis, meningitis in newborn infants, who may acquire infection from colonized mother -number declining with intrapartum antibiotic prophylaxis |
|
|
Group B Strep-pathogenesis
|
-adhere to vaginal epithelial cells, resist mucosal immune defenses
-ascent into amniotic cavity penetrating placental membranes -chorioamnionitis, bacterial proliferation allow bacteria to enter fetal lung through aspiration of infected amniotic fluid -infant can also acquire organism on passage through birth canal. -gain access to bloodstream through endothelial cells of alveoli. -neonatal serum-less efficiently opsonized, phagocytosed -polysaccharide capsule has inhibitory effect of phagocytic clearance by preventing complement deposition on bacterial surface -bloodstream dissemination |
|
|
Group B Strep- treatment and prevention
|
-treat with penicillin, ampicillin, cephalosporin
-universal screening of pregnant women (35-37 weeks gestation) |
|
|
Group C and G Strep
|
-share many microbiological, clinical characteristics with Group A Strep.
-Cause isolated exudative, common source epidemic pharyngitis, cellulitis. Cause more opportunistic, nosocomial infections |
|
|
Group D Strep
|
-gut flora
-bactermia with or without endocarditis, often result of fecal contaimination -S. bovis -Eneterococci used to be in this group |
|
|
Strep pneumonia (pneumococcus)
|
-leading cause of invasive bacterial disease in children and elderly
-normally inhabits human upper respiratory tract -causes sinusitis, otitis media (infection of middle ear) |
|
|
Strep pneumonia (penumococcus)- Microbiology
|
-Gram positive, alpha-hemolytic, catalase-negative bactera. lancet shaped pairs, or diplococci
|
|
|
Strep pneumoniae (pneumococcus)- Important structures
|
-Capsule- composed of polysaccharide completely envelops the pneumococcal cells
-Cell wall- peptidoglycan, teichoic acid -Pili-surface hair-like structures are important in colonization of upper respiratory tract -Type 3 capsular polysaccharide- grow in dome-shaped, mucoid colonies- high levels of capsule production, most virulent |
|
|
Strep pneumoniae (pneumococcus)- Clinical features
|
-major clinical syndromes- pneumonaie, bactermia, mengitis
-pneumococcal pneumoniae most common clinical presentation- short incubation period (1-3 days), abrupt onset of fever, chills, rigors. Pleuritic chest pain, cough productive of mucopurulent, rusty sputum, etc -bactermia- leads to secondary complications like arthritis, meningitis, endocarditis -meningitis- headache, lethargy, vomiting, irritability, nuchal rigidity. -acute otitis media- detected in middle ear aspirates. >60% children have had at least one episode of acute otitis media. Most frequent reason for pediatric office visits in us |
|
|
Strep pneumonia- epidemiology
|
-400,000 hospitalizations from pneumococcal pneumonia
-12,000 cases of pneumococcal bactermia. -3,000 cases of pneumococcal meningitis -accounts for much of invasive pneumococcal invasive disease in young kids |
|
|
Strep pneumoniae- Risk factors
|
-Epiglottis is physical barrier separating colonized from non-colonized areas.
-Other host factors defend against introduction of organisms from upper tract to lower tract include cough reflex, mucus secretion, and ciliary elevator -cigarette smoking, asthma, COPD- impair mucociliary clearnace -stroke, alcohol, anesthesia predispose to aspiration of nasopharyngeal secretions -alcohol, steroids, renal insufficiency, and diabetes may impair neutrophil function -immunodeficiencies -splenectomy diminishes capacity for removing opsonized bacteria from bloodstream -viral upper respiratory infections may predispose to infection by impairing ciliary function, block and impair drainage. Neuraminidase activity of viruses including influenza, parainfluenza promote adherence of pneumococci -Inflammation caused by viral infection increases transcytosis through epithelial cell -Daycare centers, military camps, prisons, crowded areas |
|
|
Strep pneumoniae- historical perspectives
|
-"old man's friend"
-treated with horse serum in pre-antibiotic era -hyperimmunized horses with pneumococcal strains of specific capsular types -antibodies administered to patients to opsonize bacteria, promote phagocytosis. this is passive transfer of type-specific hyperimmune horse serum -Quellung reaction. swollen when acted by specific antibody (antiserum) -untreated patients- 5-7 days development of type-specific antibodies |
|
|
Strep pneumoniae-pathogenesis
|
-colonizes nasopharynx
-transmitted in close contact. carriages -rate of colonization seasonal with increase in mid-winter -S. pneumoniae- attaches with: cell-wall phosphocholine (ChoP)-binds to platelet-activating factor receptor (PAFr) -neuroaminidase-cleaving sialic acid on mucous membrane surfaces, exposing GlcNAc-Gal, to which pneumococci adhere more readily |
|
|
Strep pneumoniae- immunity
|
-main components of host protection against pneumocicci are serotype-specific opsonizing antibodies, professional phagocytes
-causes disease primarily by its capacity to replicate extracellularly in host tissues and induce an intense inflammatory response -capsule-deters PMNs and macrophages. -alternative pathway: serum factor D recognizes uncapsulated teichoic acids, peptidoglycan. C3b binds, then is opsin -But capsule prevents C3b from coating bacteria. C5a is released, PMNs are attracted to area but not efficient at killing bacteria until host develops capsular serotype-specific antibodies. pathogens are serum-resisting, resistant to direct killing effects of complement -major way phagocytosis- opsonization by type-specific antibodies to capsular antigens. thats why takes 5-7 days |
|
|
Strep pneumoniae- treatment and vaccines
|
treatment-penicillin, vancomycin added for very serious infection
vaccines-polysaccharide vaccines poorly immunogenic in children younger than 2 years. -but conjugation of immunogenic nonpneumococcal protein (carrier protein) to individual peneumococcal polysaccharides elicits T cell-dependent memory response. -PCV13 used nowadays |
|
|
Listeria monocytogenes- Microbiology
|
-L. monocytogenes are gram + bacilli, but can be gram-variable
-can also look like cocci, enterococci, diptheroids -5 flagella, “tumbling motility” -grow optimally at 30-37 degrees celsius -isolate on blood agar plates ---incompletely hemolytic; catalase-positive, oxidase-negative -only L. monocytogenes pathogenic for humans |
|
|
Listeria monocytogenes- Pathogenesis
|
primary site of entry through GI tract.
foodborne infection likely mean incubation period 30 days use of antacids, H2 blockers against stomach acid increases susceptibility infection of another GI organism necessary 1. antecedent GI infections reported with listeriosis 2. long incubation suggests subclinical phase, need push from another pathogen 3. listeriosis can occur after shigellosis (another GI infection) 4. listeriosis occurs after instrumentation (colonoscopy) dissemination predilection for placental, CNS tissue |
|
|
Listeria - Virulence factors
|
Listeria is intracellular pathogen
internalin (interacts with E-cadherin on epithelial cells to promote phagocytosis) listeriolysin O, phospholipases- escape intracellular killing inducing host cell actin polymerization (form filopods)- spreads from cell to cell without ever being exposed to Ab Other factors: ActA- oligoproline surface protein- induction of actin filament assmebly Siderophores- take iron from transferrin (Fe facilitates microbes’ growth) Immunity primarily cell-mediated anitbody does not play important role no increase in listeria infections amongst asplenics, complement deficiencies, Ig disorders. BUT increased risk of infection with AIDS, lymphoma, pregnant women, people taking corticosteroids |
|
|
Listeria- Epidemiology
|
Widespread
found in soil, dust, food, water, sewage, animals Sources of infection include contaminated meat, dairy, vegetables High (28%) of Listeria fecal excretion in slaughterhouse workers Human incidence highest in summer? |
|
|
Listeria- clinical manifestations
|
1. Pregnancy infections: mild in mother, but usually fetal in fetus
nonspecific symptoms-fever, chills, back pain. isolate organism from blood cultures 2. Granulomatosis infantispeticum: transmitted via placenta stillborn with disseminated abscesses, granulomas. High fatality rate 3. Listerial sepsis: experience shock, hypotension, fever. similar to gram negative organisms occurs in neonates, immunocompromised 4. Meningitis: most common manifestation low-grade fever, may not have stiff neck, bulging fontanelles (neonates). very subtle clinical presentations. neonates: failure to thrive, poor appetite CSF will contain neutrophils, mononuclear cells. glucose low in 50%; protein between 100 and 300 mg/ml. 5. Focal infections (localized) hematogenous dissemination: skin,"", ocular, lymph nodes, hepatitis, osteomyelitis, prosthetic joint infections, spinal or brain abscess, peritonitis, cholecystitis, subacute bacterial endocarditis |
|
|
Nocardia- Microbiology
|
aerobic, gram+ bacteria, although some can be acid fast
branch into filaments, hyphae shaped light orange colonies, can be cream to yellow to brick red >50 species, half are human or animal pathogens important ones: N. abscessus, N. brasilensis, N. farcinica, N. transvalensis, N. otitidiscaviarum, N. asteroides (80% of human infections of Nocardia) |
|
|
Nocardia- Pathogenesis
|
Routes: respiratory tract (most common), direct trauma, GI
1. facultatively intracellular, can evade immune system 2. filamentous log-phase- more difficult to phagocytose than ordinary coccoids 3. surface-associated super-oxide dismutase, increased catalase levels resist oxidative killing by macrophages neutralize phagosomal acidification Host protection: T-cell mediated immunity, need T cells to clear species from lung, prevent extra-pulmonary dissemination activated macrophages trigger cell-mediated response. then direct lymphocyte-mediated destruction CNS nocardiosis- escape from lung to bloodstream. Tropism for cerebral tissue |
|
|
Nocardia- Epidemiology
|
Acquire from environment. found in soil, decaying plant material, dust, beach sand, soil, swimming pools.
no animal to human transmission or human-to-human most common route of acquisition thru respiratory tract via aerosols 500-1000 cases in US per year, increased rate because of HIV/AIDS, advanced age, cancer, use of immunosupressants Opportunistic infection. Risk factors include: organ transplantation, cytotoxic therapy or GCs, lymphoreticular malignancy, HIV/AIDS, COPD, etc |
|
|
Nocardia- clinical manifestations
|
pulmonary nocardiosis (most common)
fever, cough, chest pain, weight loss. typically necrotizing pneumonia with cavitation. can also be endobronchial inflammatory mass, lung abscess, cavitary disease CNS infection (⅓ of Nocardia infections) should have MRI brain abscess, can mimic tumor Insidious, can lead to hemiparesiseizuresres, ataxia, coma Other manifestations: cutaneous/subcutaneous infections keratitis, endophthalmitis, retinitis, kidneys, bones/joints, pericarditis/endocarditis Mycetoma (Madura foot) chronic and deep penetrating, follows trauma, involves skin, subq tissue, fascia, bone, muscle can be caused by fungi, Nocardia, Actinomyces |
|
|
Actinomyces- microbiology
|
Gram+, non-spore forming anaerobic or microaerophilic higher prokaryotic
pleomorphic, can be diphtheroidal or filamentous. once mistaken for fungal large, white, rough colonies 14 Actinomyces species, 6 pathogenic for humans: (A. israelli, A. naeslundii, A. odontolyticus, A. viscosus, A. meyeri, A. pyogenes) |
|
|
Actinomyces- pathogenesis
|
endogenous flora of mouth.
disruption of mucosal barrier permits entry Risk factors: cervicofacial actinomycosis- jaw trauma, dental disease, oral surgery abdominal- surgery, inflammatory guy, foreign bodies (fish bones) pelvic- intrauterine device (IUD) use thoracic- aspiration Polymicrobial some differences between nocardia and actinomyces: nocardia: aerobic, immune compromised, exogenous actinomyces: anaerobic, immune competent, endogenous Progression of disease usually indolent (slow), evolves over weeks, months, years lesions soft, fluctulant. Mature lesions are “woody” and fibrous sinus tract formation- drainage includes sulfur granules (hard, yellow). |
|
|
Actinomyces- Epidemiology
|
Rare infections. 1 case/300,000. More cases in men (3:1).
Found as endogenous flora in mouth. Actinomyces not found in environment, Humans only reservoir |
|
|
Actinomyces- clinical manifestations
|
cervicofacial actinomycosis (>50% cases)
poor dentition, chronic tonsillitis, otitis, mastoiditis, dental manipulation. painful pyogenic abscess. can go to “lumpy jaw” thoracic actinomycosis (lungs, pleura, mediastinum, chest wall) aspiration of oral or GI contents, or spread from cervicofacial/abdominal infections. can present as chronic pneumonia or endobrachial mass abdominal actinomycosis - very indolent occurs following penetraint trauma, surgery predeliction for involevement of iloececal region pelvic spreads from abdominal (goes to right ovary 80% of time because from ileocecal region) endometrial actinomycosis- association of IUD, septic abortion, retained sutures CNS actinomycosis brain abscess. can present as meningitis, meningoencephalitis, subdural empyema, epidural abscess |