Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
- 3rd side (hint)

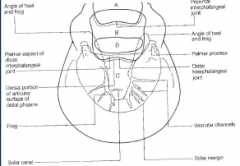
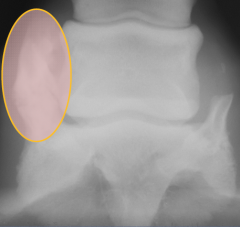
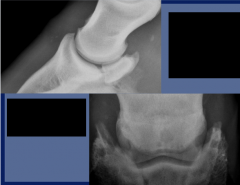
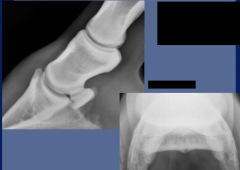
Phalanges
|
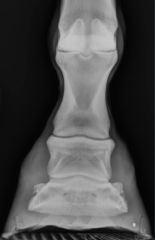
P2 is 2/3 length of P1
coffin joint is twice as wide as the pastern joint ridge on the dorsal surface of P2 is normal |
Distal interphalangeal joint is wider than the proximal interphalangeal joint
area devoid of trabeculation in the center portion of P1 and P2 that represents a marrow cavity |
|
|
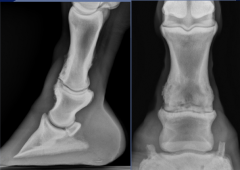
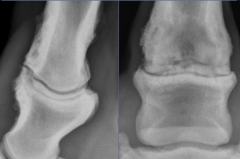
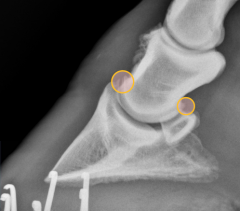
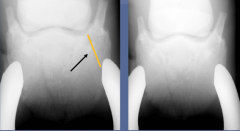
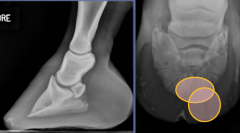
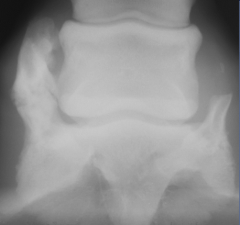
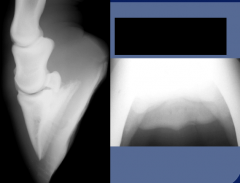
Degenerative Joint Disease
aka Ringbone -secondary to chronic repetitive trauma, fracture, infection or OC -mild to severe lameness .exacerbated with lower limb flexion -radiographic findings .joint space collapse (worse on medial) .sclerosis .osteophytes/enthesophytes .periosteal bone production .joint distention |

|
|
|

degenerative joint disease
|
|
|
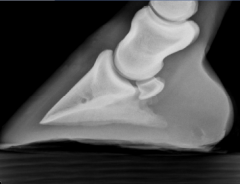
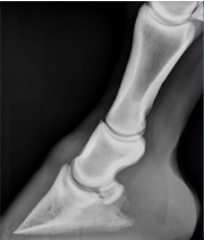
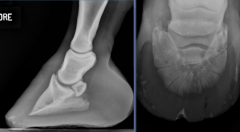
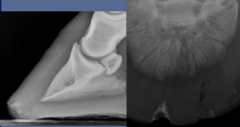
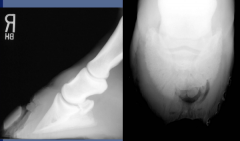
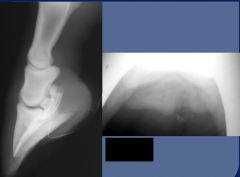
distal phalanx
coffin bone, pedal bone, P3 |
to avoid confusion artifacts, remove shoe, clean and pack foot evenly
lateromedial view |
|
|
|
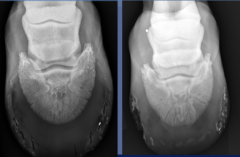
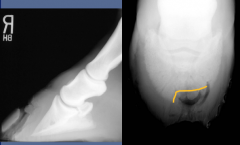
normal variation in extensor process
|
|
|
|
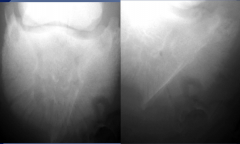
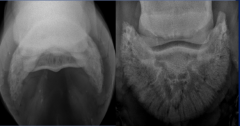
Dorsoproximal Palmarodistal View
|
High coronary stand on route
-45 degrees: projects proximal border and extremities -65 degrees: projects both borders and extremities Upright pedal route -90 degrees: projects proximal border and extremities -80 degrees: projects both borders and extremities |
|
|

|
high coronary stand on route
|
|
|
|
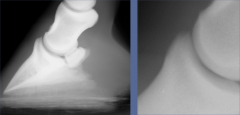
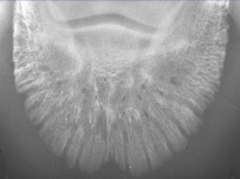
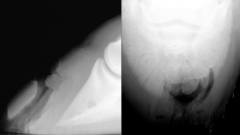
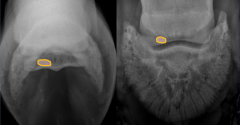
normal crena
|
|
|
|
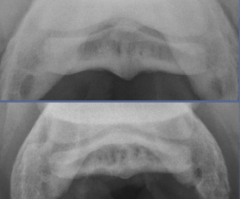
artifacts associated with packing
|
|
|
|
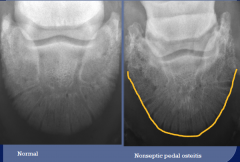
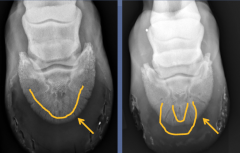
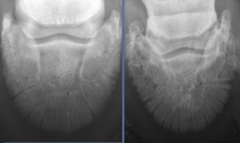
pedal osteitis complex
poorly defined complex that refers to nonspecific inflammation of P3 poor correlation to lameness changes may be permanent radiographic findings: -modelling changes of the solar margin -discrete circular lucent regions in the palmar processes - widening of the vascular channels - marginal irregularity |
|
|
|
septic pedal osteitis
puncture wound or sole abscess radiographic findings: -discrete areas of osseous lysis - irregular margin - decreased opacity - gas within the soft tissues |
|
|
|
sequestrum
secondary to septic pedal osteitis |
|
|
|
keratoma
most common tumor of the foot keratin producing tissue growing between hoof wall and coffin bone usually starts near the coronary band but can be anywhere radiographic findings -focal radiolucent defect at the solar margin (resorption) -sclerotic rim is frequently seen which aids in differentiating this from infectious process |
|
|

|
ossification of collateral cartilages
usually not clinically significant most common in draft breeds radiographic findings: -edge of ossified collateral cartilage extends beyond proximal margin of navicular bone -asymmetric mineralization - increased stress -radiolucent linear defect separate ossification center -fractures are unusual |
|
|
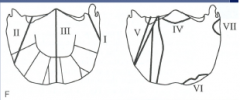
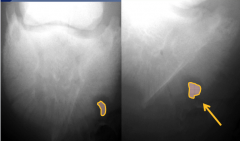
fractures
|
trauma most common cause
pathologic fractures -laminitis -septic osteitis fracture needs to be tangential to the bean better visulaization in 7 - 10 days due to rarefaction may heal without complete bony union |
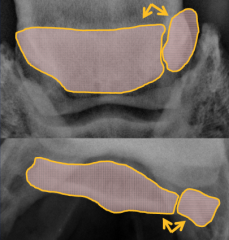
Type 1 - nonarticular fracture of palmar or plantar process
II - articular fracture, extending from distal interphalangeal joint to solar margin III - articular fracture, midsagittal, divides distal phalanx into equal parts IV - articular fractures, extensor process V - articular fractures, comminuted body fracture (not of type II, III, or IV) VI - solar margin fracture VII - palmar process fracture in foals |
|

|
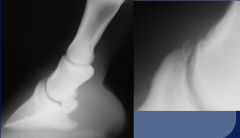
Type 1 fracture
|
|
|
|
type IV fracture
|
|
|

|
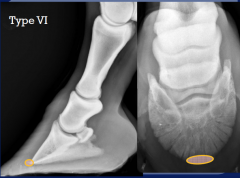
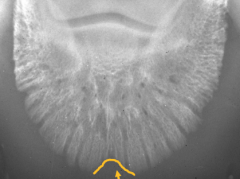
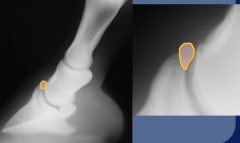
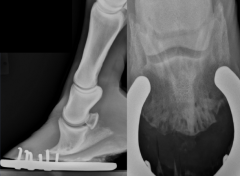
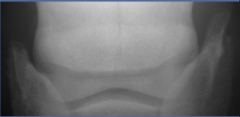
type VI fracture
|

|
|

|

Laminitis
numerous theories to etiopathogenesis inflammation and separation of laminae -dorsal hoof wall thickening -separation of dermal and epidermal lamina -rotation of P3 - lucent line clinical - acute or chronic based on presence of rotation and/or sinking |

radiographic findings:
thickening of dorsal soft tissues -greater than 20 mm lipping of distal aspect of P3 -osseous resorption -type VI solar margin fractures rotation -palmar rotation radiolucent line between P3 and hoofwall -necrosis, gas, infection thin sole -convex bulge on contour of the sole sinking -distal displacement of P3 |
|
|
chronic laminitis:
changes to conformation and contour of 3rd phalanx "slipper toe" |
|
|
|
high coronary (60 degree DP)
-centered slightly above coronary band used to evaluate the synovial invagination, wings of navicular bone, attachment sites of the impar ligament and collarteral ligaments |
|
|

|
Flexor Skyline
used to evaluate the flexor surface, corticomedullary distinction, and number of synovial invaginations |
|
|

|
Bipartite navicular bone
two centers of ossification (bi or tri partite/bilateral or unilateral) degeneration of navicular bone and source of lameness can look just like chronic fracture healed by fascial union can be incidental -60 degree DP view |
|
|
|
Palmar Heel Syndrome, Navicular syndrome, navicular degeneration
|
clinical syndrome associated with pain arising from the navicular apparatus
-navicular bone -impar ligament -DDFT -collateral sesamoidean ligaments -navicular bursa -distal interphalangeal joint -third phalanx (P3) secondary process, concurrent process - soft tissue structures affected no universally accepted defintion based on pathological or radiographic findings -clinical condition causing progressive forelimb lameness which is not permanently alleviated by rest or corrective shoeing - controversy over the significance of radiographic changes in navicular bone |
Radiographic findings
-proximal border: enthesophytes (at attachement of sesamoid collateral ligament and suspensory navicular lig), modelling - distal border: (60 degree DP view)s ynovial invaginations, small osseous fragments (at attachment of impar lig) - flexor cortex: (navicular skyline view, lateral view) cortical erosions, mineralization of the DDFT - medullary cavity changes: cysts, sclerosis (reduction in corticomedullary differentiation) there is correlation with clinical lameness and flexor cortex erosions, medullary cysts, and sclerosis of navicular bone |
|
|

Navicular degeneration
proximal border and distal border changeschanges enthesopathy collateral sesamoidean ligament reduction in corticomedullary distinction distal border enlargement of synovial invaginations cyst dystrophic mineralization of DDFT sharp contour of margin |

concave contour of bone, smoothly marginated
avulsion bone fragment large cyst in navicular bone |
|
|
Navicular degeneration
navicular skyline and 60 degree DP view changes in synovial invaginations avulsions, smooth margin, overlying medullary cavity of navicular bone |
|
|
flexor surface erosions
|

medullary cysts
60 degree DP view |
medullary sclerosis
lateral view, skyline view |
|
|
Infection
secondary to puncture wound (nail, foreign object) radiograph may be normal at time of injury - if recent possibly seen avulsion fracture additional imaging with positive (iodinated) contrast agent should be considered (sinography) penetrating soft tissue, or synovium later in disease: (aggressive disease process) -destruction of flexor cortex -lysis of navicular bone -sclerosis |
|