Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
91 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
List the pathology and diseases that occur secondary to luminal narrowing/obstruction
|
Atherosclerosis, thrombosis, emboli
|
|
|
|
List the pathology and dz that occur secondary to weakening of the vessel walls
|
Dilation, dissection, rupture
|
|
|
|
List the 5 important pathological processes of blood vessesl
|
1. Athersclerosis (most important according to Nowacki)
2. Vasculitis (div by type) 3. Aneurysms 4. Diseases of Veins 5. Blood vessel neoplasms |
|
|
|
what are the vessel layers
|
Intima, internal elastic lamina, media, external elastic lamina, adventitia
|
|
|
|
how does arterial wall thickness change as vessels become smaller
|
wall thickness decreases but the ratio of thickness to lumen diameter increases
|
|
|
|
how are vessels classified according to size
|
large = elastic
medium = muscular small = <2 mm arterioles = 20-100 micrometers capillaries = 7-8 microns |
|
|
|
which vessel is the principle point of physiologic resistance
|
arterioles
**important point of involvment in HTN |
|
|
|
what is the relationship between diameter and resistance
|
la place's law --> wall tension is proportional to diameter and internal pressure in lumen
as diameter decreases by 1/2, resistance increases by 16 |
|
|
|
what is the vasa vasorum and where is it found?
|
small vessels to supply the outer portion of media in large vessles
* important in syphillis |
|
|
|
where are the nerves found?
|
in the adventitia
|
|
|
|
what is the difference between between capillaries and arterioles
|
1.size
2.capillaries have endothelium cell lining as well, but lack media. 3.capillaries have a larger cross section and thinner walls to give a slower flow and rapid diffusion fact from notes: capillaries allow for rapid exchange and diffusion from vessels to tissue and vice versa |
|
|
|
what are the two types of capillaries
|
continuous and fenestrated
|
|
|
|
where are capillaries most dense
|
in metabolically active tissue (ie heart)
|
|
|
|
what size vessels are most affected by HTN
|
arterioles
|
|
|
|
what size vessles are most affected by Atherosclerosis
|
large arteries
|
|
|
|
what does ectasia mean
|
vascular dilation, +/- tortuosity
|
|
|
|
where does vascular leakage and leukocyte excudation (inflammation escape vessels) occur
|
post capillary venules
|
|
|
|
why are venules, veins, and lymphatics more subject to injury and invasion by cancer
|
because they are thinner, less organized, and there is less structure
|
|
|
|
list the layers of the large veins, medium veins, venules, post capillary venules
|
They all have an intima, media, and adventitia
|
|
|
|
what is present in the large and muscular arteries that is not present in the arterioles and capilaries
|
elastic lamina
|
|
|
|
what surrounds the capillary endothelium
|
pericytes
|
|
|
|
Due to the poor support of veins, list three things they are predisposed to
|
veins are predisposed to 1.irregular dilation 2.compression
3.easy penetration by tumors and inflammatory processes |
|
|
|
Lymphatics are thin, endothelial lined channels that drain interstial fluid and inflammatory cells back to the blood.
|
Lymphatics constitute an important pathway for disease dissemination through transport of bacteria and tumor cells to distant sites.
|
|
|
|
List the congenital vascular abnormalities
|
1. Congenital Heart Disease
2. AV fistulas 3. Developmental or Berry Aneurysms 4. Fibromuscular Dysplasias (renal artery dysplasia |
|
|
|
AV Fistulas
|
They occur most commonly as developmental defects but can also result from rupture of an arterial aneurysm into an adjacent vein, from penetrating injuries that pierce arteries and veins, or from inflammatory necrosis of adjacent vessels; intentionally created arteriovenous fistulas are used to provide vascular access for chronic hemodialysis. Like berry aneurysms, ruptured arteriovenous fistulas can be an important cause of intracerebral hemorrhage.7 Large or extensive arteriovenous fistulas become clinically significant by shunting blood from the arterial to the venous circulations and forcing the heart to pump additional volume; high-output cardiac failure can ensue.
|
|
|
|
Berry Aneurysms
|
occur in cerebral vessels; when ruptured these can be causes of fatal intracerebral hemorrhage
|
|
|
|
Fibromuscular Dysplasias
|
focal irregular thickening of the walls of medium and large muscular arteries, including renal, carotid, splanchnic, and vertebral vessels. The cause is unknown but is probably developmental; first-degree relatives of affected individuals have an increased incidence. Segments of the vessel wall are focally thickened by a combination of irregular medial and intimal hyperplasia and fibrosis; this results in luminal stenosis, and in the renal arteries may be a cause of renovascular hypertension Vascular outpouchings (aneurysms) may develop in the vessel segments with attenuated media and in some cases can rupture. Fibromuscular dysplasia can manifest at any age, although it is seen most frequently in young women; there is no association with use of oral contraceptives or abnormalities of sex hormone expression
|
|
|
|
From Table 11- 1 (stated this table isn't important, but it is for test taking -- i guess meanign boards so i included it)
Elaboration of anticoagulant, antithrombotic, fibrinolytic regulators |
prostacyclin
thrombomodulin heparin- like molecules plasminogen activator |
|
|
|
table 11-1 elaboration of prothrombotic molecules
|
vWF
tissue factor plasminogen activator inhibitor |
|
|
|
table 11-1 modulation of blood flow and vascular reactivitiy
|
vasoconstrictors; endothelin and ACE
vasodilators: NO, prostacyclin |
|
|
|
table 11-1 Regulation of inflmmation and immunity
|
IL-1, IL-6, chemokines
adhesion molecules, VCAM -1, ICAM, E-selectin, P-selectin histocompatibility antigens |
|
|
|
table 11-1 regulation of cell growth
|
stimulators: PDGF, CSF, FGF
inhibitors: heparin, TGF-B |
|
|
|
from table 11-1 other things that maintain the permeability barrier
|
oxidation of LDL
extracellular matrix production (collagen and proteoglycans) |
|
|

table 11-2 for review
|
list the causes of endothelial dysfunction
|
turbulent flow, HTN, cytokines, complement, bacterial products, lipid products, advanced glycation end products, hypoxia, acidosis, viruses, cigarette smoke
|
|
|
compare the amount of blood in the veins vs the arteries
|
2/3 of the blood is contained in the veins
|
|
|
|
where is vWF stored
|
in weibel-palade bodies (membrane bound storage organelles) in endothelial cells
|
|
|
|
what immunohistochemical stains ID endothelial cells
|
CD31, CD34(PECAM1), factor VIII and vWF
|
|
|
|
what factors promote vascular smooth muscle cell growht
|
PDGF, endothelin-1, thrombin, FGF, INF-gamma, IL-1, vascular injury, endothelial cell dysfunction or loss
|
|
|
|
what factors inhibit vascular smooth muscle cell growth
|
heparin sulfates, NO, TGF-B
|
|
|
|
Vasoconstrictors
|
endothelin, angiotensin II, catecholamines, alpha adrenergic factors, thromboxane, leukotrienes
|
|
|
|
vasodilators
|
NO, kinins, prostaglandins, natriuretic peptides, beta adrenergics factors
|
|
|
|
what deactivates NO
|
free radicals produced by macrophages and endothelial cells (also cause oxidation of LDL)
|
|
|
|
what are the 5 functions of vascular smooth muscle cell
|
1. vasoconstrict
2. vasodilation 3. make extracellular matrix proteins 4. make growth factors and cytokines 5. can migrate and proliferate |
|
|
|
vascular injury = smooth muscle stimulation and growth
describe the healing process |
1. smooth muscle cells migrate to the intima, loose the ability to contract, and gain ability to divide
2. smooth muscle cell mitosis 3. elaboration of extracellular matrix ** results in intimal thickening-->will duplicate and triplicate the internal elastic lamina until there is no lumen |
|
|
|
what are the functions of the contractile phenotype of the vascular smooth muscle
|
vasoconstriction/dilation
|
|
|
|
what are the functions of the profliferative/synthetic pheontype
|
connective tissue proteins, growth factors, cytokines
- blood vessel repair and atherosclerosis |
|
|
|
what are the 3 patterns of arteriosclerosis
|
1. atherosclerosis
2. monckeberg medial calcific sclerosis 3.arteriolosclerosis |
|
|
|
define arteriosclerosis
|
thickening and loss of elasticity of arterial walls
|
|
|
|
Describe atherosclerosis
|
*most frequent and most important
*slowly progressive dz of intima of large to medium sized muscular and large elastic arteries * atheromatous plaques that protrude into and obstruct vessel lumen *weakend media due to loss of internal and external elastic membrane |
|
|
|
Descending order of frequency in atheroslerosis
|
abdominal aorta > coronary arteries > descending thoracic aorta > internal carotid arteries > circle of willis
|
|
|
|
characterize and atheroma
|
a fibrofatty plaque that protrudes into and obstructs vascular lumens along with weakening of the underlying media
|
|
|
|
Other random facts about atherosclerosis from notes
|
- accounts for 1/2 deaths in western countries (MI, Stroke, PVD, aneurysms)
- asymptomatic for long time - can be completely or partially obstructed --> for the heart takes approx 70% to be affected -clot or hemorrhage lead to MI |
|
|

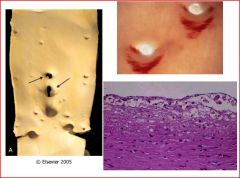
what is this a picture of
|
describe the typical findings
|
- calcific deposits in muscular arteries in people >50.
-may be seen on xray or palpated **no significant clinical sequelae -muscle is replace by Ca, media and elastic are fine. -does not encase the entire artery (different than atherosclerosis) |
|
describe this pathology
|
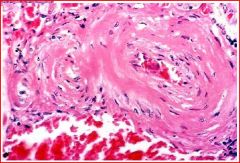
this is hyaline arteriosclerosis, what are the characteristics
|
pink homogenized thickening with vessel lumen (hyalinized, no cells) narrowing in elderly (+/- HTN) and in diabetics (microangiopathy)
|
|
describe the pathology
|
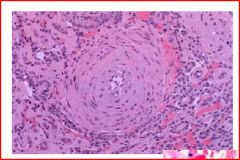
this is hyperplastic arteriolosclerosis, describe its characteristics
|
onion skin concentric thickening with narrowing of the vessel lumen, seen in really high HTN (malignant)
|
|

describe the natural history of atherosclerosis after reviewing this image
|
normal vessel-->fatty streak-->fibrofatty plaque-->advanced vulnerable plaque
Now describe the clinical phases of the vulnerable plaque |
1. mural thrombosis, embolization, and wall weakening -->aneurysm and rupture = hemorrhagic stroke
2. plaque rupture, plaque erosion, plaque hemorrhage, mrual thrombosis, emoblization-->occlusion by thrombus = MI, stroke 3. progressive plaque growth -->critical stenosis = claudation, angina |
|
|
Describe fatty streaks; when does it first appear, where does it develop, is it related to atheroclerosis
|
1. is is the earliest atherosclerotic lesion --> appear in all children by age 10
2. often occur in vascular regions that later in life DONT develop atheromas 3. may be related somehow but true relationship not yet defined |
|
|
|
name the common complications of atherosclerosis
|
MI, stroke, aortic aneurysms, PVD, diminished arterial perfusion, mesenteric occlusion(60, 70 yo), chronic ischemic heart dz
|
|
|
describe the morphology
|
raised white, yellow intimal based lesion with prominence around ostia of majro branches,
picture in upper R has the fat stain added, see fattty streak around origin image in lower R demonstrates fatty plaque with intimal macrophage derived foam cells |
|
|
|
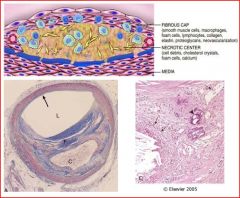
describe the plaque composition
|
superficial fibrous cap (sm mus, leukocytes, dense CT ECM, collagen, elastin, proteoglycans, neovasculization)
necrotic lipid laden core (cell debri, foam cells, cholesterol clefts &/or crystals, dead cells, calcium) periphery has neovasculization *often undergo calcification |
|
|

Figure 11-12 Gross views of atherosclerosis in the aorta. A, Mild atherosclerosis composed of fibrous plaques, one of which is denoted by the arrow. B, Severe disease with diffuse and complicated lesions (with plaque rupture and superimposed thrombosis), some of which have coalesced.
|
A and C are included :
Histologic features of atheromatous plaque in the coronary artery. A, Overall architecture demonstrating fibrous cap (F) and a central necrotic (largely lipid) core (C). The lumen (L) has been moderately compromised. Note that a segment of the wall is free of plaque (arrow); the lesion is therefore "eccentric". In this section, collagen has been stained blue (Masson's trichrome stain). B, Higher power photograph of a section of the plaque shown in A, stained for elastin (black), demonstrating that the internal and external elastic membranes are attenuated and the media of the artery is thinned under the most advanced plaque (arrow). C, Higher magnification photomicrograph at the junction of the fibrous cap and core, showing scattered inflammatory cells, calcification (arrowhead) and neovascularization (small arrows). |
|
|

Right: thrombus can rapidly progress to full occlusion
Left: Calcium can overtime turn into bone |
more atherosclerosis slides
|
|
|
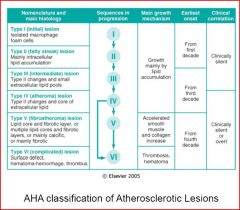
AHA Classification
|
review to the level you think will be good for the test
|
|
|
|
describe type II lesions
|
- fatty streak that is not raised, 1mm to 1 cm, and includes intracellular lipid accumulations and T lymphocytes
-occur at sites that are (and are not) susceptible to atheroma formation |
|
|
|
what levels of vessels are affected by plaques
|
elastic - aorta, iliac, carotid
muscular - coronary, popliteal |
|
|
|
what events lead to advancement of plaque
|
cell death, inflammation, plaque growth, remodeling of plaque, organization of thrombus, calcification
|
|
|
|
what events lead to fatty streaks & stable plaques (ie early natural history)
|
endothelial dysfunction, monocyte adhesion, SMC migration, SMC proliferation, ECM elaboration, & lipid accumulation
|
|
|
|
what are the four modifiable risk factors for atherosclerosis
|
1. hyperlipidemia - diet
2. hypertension - decrease salt intake, Rx 3. cigarette smoking - QUIT! 4. diabetes |
|
|
|
what are the 4 non-modifiable risk factors for atherosclerosis
|
age
male gender (until women are post menopausal) family hx genetic abnormalities |
|
|
|
Other random risks of atherosclerosis
|
obesity, type a personality, alcohol, LP(a), post menopausal estrogen deficiency, high carb intake, physical inactivity, chlamydia pneumoniae, increased serum homocysteine
|
|
|
|
what type of infections may predispose to atherosclerosis
|
chlamydia pneumonia and CMV (because they infect the endothelial cell)
|
|
|
|
which cholesterol is associated with increased risk of atherosclerosis
|
LDL (delivers cholesterol to peripheral tissues)
|
|
|
|
what is the most important factor in atherosclerosis
|
hypercholesterolemia --> less than 150mg/dl =low risk
|
|
|
|
why is HDL a good cholesterol
|
it mobilizes cholesterol from the existing atheroma and transports it to the liver for excretion in bile
-random drug mentioned Gemfibrozil (sp?) - reduces triglycerides and increases amt cholesterol carried in HDL |
|
|
|
what 3 things raise HDL
|
exercize, moderate alcohol, weight loss, QUIT smoking
|
|
|
|
how do statins lower cholesterol
|
by inhibiting HMGCoA reductase (req for cholesterol synth in liver)
|
|
|
|
what inborn error in metabolism predisposes to vascular dz
|
homocysteinuria (high levels of homocysteine > 100umol/L
|
|
|
|
what dietary defect can cause homocysteinuria
|
low folate and vit B12 intake
|
|
|
|
what cirulating markers are predictors of athero risk
|
plasminogen activator inhibitor-1 (PAI-1), CRP, lipoprotein a (LPa)
|
|
|
|
how does lipoprotein a LPa differ from LDL
|
lp(a) contains apolipoprotein B-100 of LDL linked to apo-A
|
|
|
|
what type of flow may lead to endothelial dysfunction
|
turbulent flow with low shear stress
|
|
|
|
what binds t cells and monocytes to cause formation of atheroma
|
VCAM-1
|
|
|
|
what do macrophages produce that increases adherance of WBCs
|
IL-1 and TNF
|
|
|
|
what defect is present in homozygous familial hypercholesterolemia
|
defects in the LDL receptor
resulting in decreased hepatic uptake and increased circulating LDL - LDL 5-10 X normal =severe atherosclerosis in childhood these patients may have MI before age of 20 |
|
|
|
describe heterozygoes for familial hypercholesterolemia
|
LDL cholesterol 2-3X normal, decreases hepatic uptake of LDL/IDL and premature atherosclerosis, Xanthomas
|
|
|
|
Hyperlipoproteinemias
Type IIa |
High Chol HIgh LDL
defect: LDL rec or Apolipoprot E |
|
|
|
Hyperlipoproteinemias
Type IIb |
High Chol&Triglyceridesm High LDL & VLDL
defect: LDL rec or Apolipoprot B |
|
|
|
Hyperlipoproteinemias
Type IV |
High Triglycerides High VLDL
Defect: lipoprotein lipase |
|
|
|
Describe the response to Injury Hypothesis
|
Atherosclerosis is a chronic inflamatory response of the arterial wall initiated by injury to the endothelium. Lesion progression is sustained by interaction between modified lipoprotiens, monocyte derived macrophages, T lymphocytes, and normal cellular constituents of the arterial wall
|
|
|
|
Describe the pathogenesis and progression to plaque formation
|
chronic endothelial injury--> lipoprot (LDL/VLDL) & lipids gain entry into vessel wall and acculuate (right under endothelium)--> monocytes and platelets attach, mono's migrate into intima and transform inot macro and then foam cells--> migration and prolif of SMCs--> ongoing lipid accumulation and growth of plaque -->creates a bump in vessel wall --> creates more turbulence--> back to begining again with more endothelial injury
|
|
|
|
what are the causes of endothelial injury
|
hyperlipidemia
smoking hypertension immune attack distrubed flow (turbulence) toxins **Injury more prone at sites with turbulent blood flow |
|