![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
224 Cards in this Set
- Front
- Back
|
What percent of the population have a speech and/or hearing disorders? |
10-15% |
|
|
Incidence |
Number of new cases per certain time period |
|
|
Prevalence |
Number of cases present at a certain time |
|
|
Sensitivity |
A tests ability to identify positive results Sn = TP/(TP + FN) |
|
|
Specificity |
A tests ability to identify negative results Sp = TN/(TN+FP) |
|
|
Oto - |
ear |
|
|
-itis |
infection/inflammation |
|
|
-algia |
pain |
|
|
-rrhea |
fluid |
|
|
-ectomy |
remove/excise |
|
|
-otomy |
cut into/incise |
|
|
-plasty |
alter or change |
|
|
Hypo- Hyper- |
too little too much |
|
|
Tumor Lesion |
any growth or mass skin changes, masses |
|
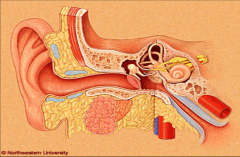
Outer Ear |
Auricle (pinna, outer ear) External auditory canal (EAC) - outer 40% cartilaginous (skin, hair and sebaceous glands overlay cartilagenous portion), inner 60% is bony and lined with skin sebaceous glands produce wax for protection narrowest point at bony-cartilaginous junction (isthmus) * some syndromes present with altered position of the ear - should be at eye level and have slight back tilt |
|
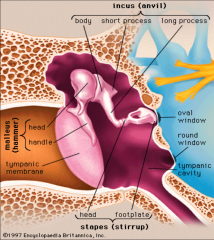
Middle Ear |
Tympanic membrane Ossicles (malleus, incus, stapes) |
|
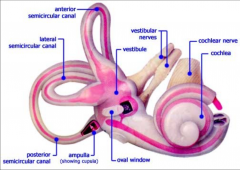
Inner Ear |
Cochlea Balance organs (SSCs and vestibular organs) * membranous labyrinth (endolymph) is within bony labyrinth (perilymph is in between) Medial from inner ear is CN8 (cochleovestibular nerve) which attaches to the cochlea and semicircular canals |
|
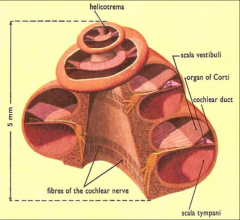
Cochlea |
2.5 turns
|
|
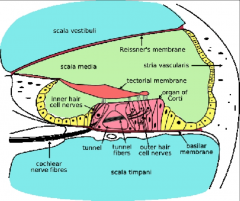
Organ of Corti |
Mechanical energy of cilia on hair cells moving is transferred into nerve firing (electrical energy) IHC, OHC, tectorial membrane |
|
CAS |
Any interruption in signal transmission from outer ear to auditory cortex is a hearing disorder |
|
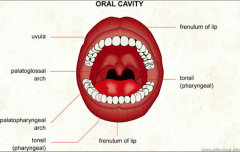
Oral Cavity What is done in a mouth and throat exam? |
bright light is important use tongue depressor to view throat, tongue and all mucosal surfaces press on only anterior 1/2 of tongue |
|
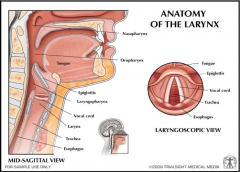
Larynx |
Endoscopic assessment |
|
|
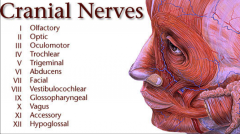
I - smell II - vision III - eyelid and eyeball movement IV - turns eye inferiorly and laterally V - mastication, touch/pain of face VI - turns eye laterally VII - facial expression, secretion of tears and saliva, taste VIII - hearing, equilibrium IX - taste, throat sensation, carotid blood pressure X - aortic blood pressure, heart rate, digestive organs, vocal cords, swallowing XI - trapezius and sternocleidomastoid, swallowing XII - tongue movement - will deviate to side opposite lesion
|
|
|
Patient Evaluation |
History - present illness (otological or speech), past medical/surgical history, medication/allergies, family history, birth history, otological history, Physical examination - ear inspection (masses, skin changes, symmetry, abnormal shape or position, discharge) otoscope (examine EAC, TM and middle ear space - use largest size speculum that fits, gently pull ear back and point otoscope in sup/ant direction), exam of swallowing mech and articulators Investigations/tests (audiogram, speech and language tests) Diagnosis Treatment and referral Follow up |
|
|
Otoscopy accuracy |
41% accuracy among paediatric residents and 51% among pediatricians in diagnosis of AOM
35/135 children diagnosed with AOM by GP had no middle ear effusion |
|
|
2 other kinds of otoscopy |
Pneumatic otoscopy Otomicroscopy |
|
|
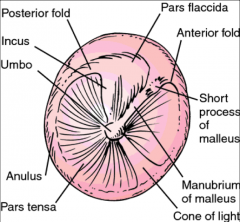
What to look for in Otoscopy |
EAC abnormalities pars tensa pars flaccida color/thickness of TM translucency anatomic structures |
|
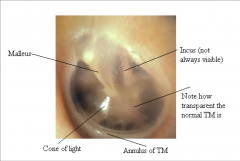
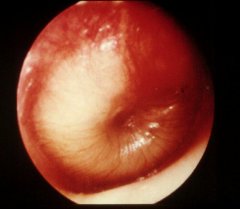
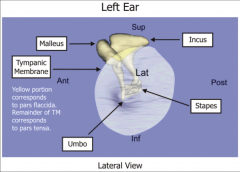
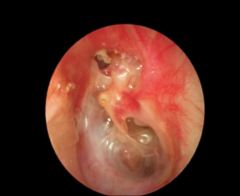
Which ear is this? what should be identified? |
Left TM identify malleus (umbo, lateral process, handle), cone of light, pars tensa, pars flaccida, long process of incus |
|
|
What are the 2 tuning for tests? How are they done? What frequency tuning fork are they done with? |
Weber - push tuning fork down firmly at midline of forehead Rinne - hold tuning fork on mastoid bone and then in front of ear. 512 Hz tuning fork |
|
|
What is determined from the Weber test? |
Uses the occlusion effect - if it lateralizes to the right it indicates conductive hearing loss on right side or SNHL on left OR vice versa
Normal = no lateralization |
|
|
What is determined by the Rinne test? |
Normal - AC > BC (Rinne +ve) CHL - AC < BC (Rinne -ve) SNHL - AC >BC (Rinne +ve) |
|
|
What are the different dB? |
dB HL - threshold dB based on normative hearing data as a reference. 0 dB HL is the minimal intensity for average ear to perceive a specific frequency dB SL - level in dB above an individuals threshold |
|
|
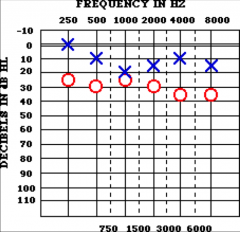
What are the 3 measures on an audiogram? |
pure tone testing - frequency response, ability to detect sound speech testing - ability to decode sound acoustic impedance - helps define where problem is. Tested in tympanometry |
|
|
What frequencies (pure tones) are assessed in pure tone testing? |
250, 500, 1000, 2000, 4000, and 8000 HZ |
|
|
Parts of an air conduction audiogram What is assessed in AC? |
lowest level dB HL at which the subject perceives 50% of pure tones introduced via earphones or speakers (sound field) conduction from auricle to cochlea |
|
|
Parts of a bone conduction audiogram What is assessed in BC? |
lowest level dB HL at which the subject perceives 50% of pure tones introduced via bone oscillator conduction from skull bones to cochlea (bypassing the EAC and middle ear) |
|
|
What is the pure tone average (PTA) based on? |
average threshold at 500, 1000 and 2000 Hz should be within 10dB of speech reception threshold |
|
|
What is the speech reception threshold (SRT)? |
lowest dB HL patient can repeat a spondee 50% of the time |
|
|
What is the speech discrimination score (SDS)? |
% of phonemes repeated correctly after being presented at 20-40dB SL above SRT |
|
|
What is the air bone gap (ABG) |
decibel difference between BC and AC |
|
|
What is a conductive hearing loss? What is a sensorineural hearing loss? What is a mixed hearing loss? |
CHL: normal BC with abnormal AC (ABG), maximal CHL is 60dB SNHL: abnormal bone conduction conduction and as a result abnormal AC, no ABG mixed: abnormal AC and BC with small ABG |
|
|
What is recruitment? What disorder does it suggest? |
increasing signal intensity leads to out-of-proportion perception of loudness
suggests cochlear hearing loss e.g. endolymphatic hydrops |
|
|
What is rollover? What disorder does it suggest? |
paradoxical decrease in discrimination ability with increasing stimulus intensity
suggests retrocochlear disorder e.g. acoustic neuroma |
|
|
What is tone decay and fatigue? What disorder does it suggest? |
decrease in auditory perception with a sustained stimulus
suggests retrocochlear disorder |
|
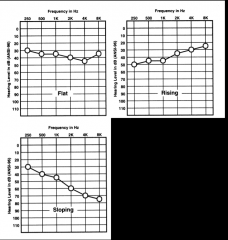
Name the types of hearing loss |
flat rising slopping cookie bite |
|
|
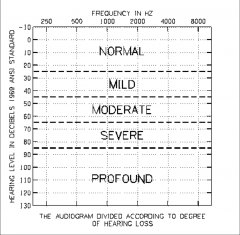
What are the ranges in severity of hearing loss? |
|
|
|
What is masking and crossover? |
Masking: noise introduced with AC into non-test ear to prevent crossover. usually white noise Crossover: perceived sound from an acoustic signal introduced to opposite ear the more intense the stimulus the more likely to have cross over. AC crossover occurs when test ear intensity is 40dB/50dB or greater than BC of non-test ear. BC crossover occurs at 0dB |
|
|
What is the masking dilemma? |
When enough masking to prevent crossover is overmasking Bilateral ABG of 50dB cannot be masked |
|
|
How is acoustic impedance tested? |
Tympanometry: transmission/reflection of sound energy. Plots compliance changes of TM vs air pressure in the EAC. Max compliance should be near 0 pressure range. Hole in TM indicated by too much compliance and liquid behind TM is indicated by too little compliance
|
|
|
What are the types of tympanometry assessment results? |
A: normal (peak between -150 & +50 daPa As: "shallow" (reduced compliance) AD: "deep" (hypercompliant) B: flat (effusion, perforation, tube) C: -ve pressure (retracted TM, ETD) |
|
|
What muscles are involved in acoustic reflex? Why does it occur?
|
contraction of stapedial muscle in response to high intensity sound (ipsilateral and contralateral responses, ipsilateral > contralateral) cause bilateral contraction to prevent movement of stapes |
|
|
What is suggested by decay or absence of acoustic reflex? |
decay: retrocochlear lesion absent: minimal CHL, SNHL (>60 dB), brainstem lesion, CN VIII impairment, CN VII dysfunction |
|
|
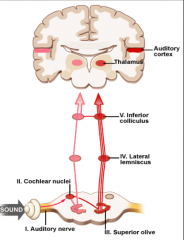
What are 4 additional audiometric tests? |
Electrocochleography (ECoG) Cochlear Potentials Otoacoustic emissions (OAE) - objective sound in the EAC emitted from outer hair cells, presence of OAE = normal cochlea. OAE normal with retrocochlear and central auditory disorders Auditory brainstem response (ABR) - recording of the activity of 8th nerve and CNS response to auditory stimulus. electrodes placed on head, mastoid, and ear to detect electrical signals with sound stimulus. ABR peaks (ECOLI). I-II eighth cranial nerve, III cochlear nuclei, IV olive(superior), V lateral lemniscus, VI-VII inferior colliculus. |
|
|
Congenital Estimates for congenital hearing loss |
trait present at birth - not always genetic - can express themselves later in life e.g. late-onset vs acquired - estimates for congenital SNHL range from 1/600 to 1/2000, congenital conductive loss is much less common |
|
|
Aquired |
not present at birth |
|
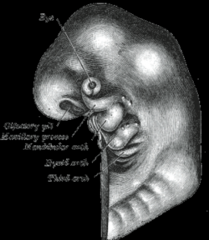
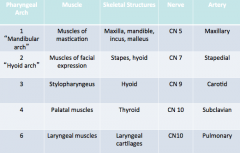
Embryology-Branchial Arches or Pharyngeal Arches - Purpose? |
bumps give rise to the head and neck neural press cells migrate from the neural tube to the front of the head/neck - will differentiate and form anatomy during embryogenesis ear formation starts in the low neck and then migrates to its proper position |
|
|
What pharyngeal arch is associated with specific skeletal structures |
|
|
|
What is a hillock of his and which arches are they associated with? |
Hillock of his = mounds of primordial tissue which fuse with each other to form the pinna 1st arch: 1-3 hillcocks of his 2nd arch: 4-6 hillocks of his |
|
|
External Ear Development |
Pinna: 1st and 2nd brachial arches, 1st arch: 1-3 hillcocks of his, 2nd arch: 4-6 hillocks of his
EAC: 1st brachial arch
|
|
|
Progression of Pinna development |
Week 6: hillocks of his distinct, start fusing Week 8: pinna structures identifiable Week 18: Pinna adult form |
|
|
Progression of EAC development |
Week 4: EAC begins Week 6: hillocks distinct Week 8: auricle identifiable structure Week 18: Auricle adult form Week 20: EAC plug disintegrates (is plugged with tissue when it develops) Week 28: EAC fully open |
|
|
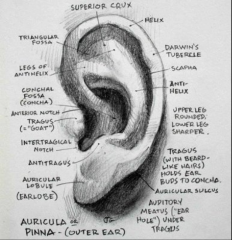
Label all the parts of the auricle |
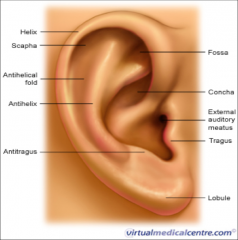
upper 2/3 is skin and cartilage, bottom 1/3 is skin and fat antihelix/antihelical rim - splits into supper crus and inferior crus and between them is triangular fossa scaphoid fossa concha bowl - superior (concha cymba) and inferior (concha cavum) tragus and antitragus |
|
|
Sensory innervation, lymphatic system and blood supply of the external ear |
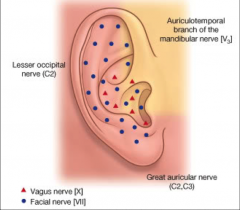
CN V, VII, IX, X and great auricular nerve (nerve that comes from the neck C2, C3)
blood supply: superficial temporal and posterior auricular arteries
lymphatics (fight infection): parotid and cervical nodes. Infections and inflammatory conditions of the EAC can present with enlarged lymph nodes |
|
|
Perichondritis/Chondritis |

Perichondritis: Inflammation/infection of perichondrium Chondritis: Inflammation/infection of cartilage. same presentation as cellulitis but lobule is spared. IV antibiotics |
|
|
Cryptotia |

superior part of helix is hidden under the skin, it is there but it is buried missing supra-aural sulcus for glasses to rest or for behind the ear hearing aids |
|
|
Cup/lop ear |
ear is constricted or folding on itself Different degrees |
|
|
Stahl ear |

Extra limb of cartilage tissue that comes from antihelix, connecting the helix to the antihelix cosmetic issue |
|
|
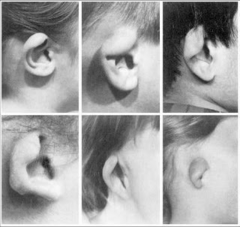
Microtia |
external ear is severely underdeveloped and malformed - mound of tissue also missing the EAC - can't hear on one side Grade 1-3 to convey how sever the microtia is Can have microtia reconstructive surgery |
|
|
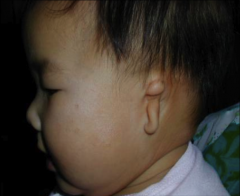
Preauricular pits |

Dimple in the skin in front of the ear, superior to EAM opening - most of the time it is a skin lined tunnel that is 1-2cm long |
|
|
Preauricular skin tags |

Most are removed when child is very young related to hillocks of his fusion - fusion is too strong and pushes skin flap out |
|
|
Darwin's Tubercle |
Bump on inside of helical rim normal varient |
|
|
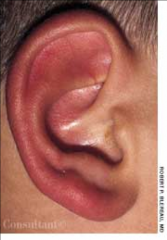
Prominent Ears Prominotia |
Top of ear and head should be about 20 degrees Underlying issue = no anti-helical fold (absent or underdeveloped) and the concha bowl cartilage is excessive or hypertrophic Psychosocial distress |
|
|
Congenital abnormal auricle - next steps? |
All abnormal auricles (except Darwin's tubercle and mild prominent ears) should be referred
Look for other congenital anomalies and syndromic features in the presence of abnormal ears
Preauricular pits and/or tags + SNHL - possibly a syndromic cause |
|
|
Auricular hematoma |

Most commonly due to trauma Collection of blood between cartilage and pericardium Can have CHL: EAC swelling, hemotympanum (middle ear blood), ossicular injury/discontinuity In children - rule out abuse Urgent referral indicated for incision and drainage |
|
|
Cauliflower ear |

Occurs secondary to hematoma auricular traum - hematoma - cauliflower ear (if hematoma left untreated) hematoma disrupts blood supply to auricular cartilage which leads to cartilage necrosis (death) and neocartilage formation
common in wrestlers and rugby players |
|
|
Cellulitis |
Inflammation/infection of skin pain (on touch) warmth erythema (redness) Edema (swelling) Pruritus (itching) weeping and crusting
treat with oral antibiotics
|
|
|
Split lobule |

typically due to earing getting ripped out |
|
|
Frost bite |
Superficial to deep erythema (light skin) or gray colour (dark skin) tingling, stinging sensation numb, yellow, waxy/shiny, gray colour feels cold, stiff, woody blisters black necrosis
immediate referral |
|
|
Sunburn |
worst in transitions from winter/summer fair skin, light hair exposed skin areas snow can reflect sunlight UV light major risk factor for skin cancer |
|
|
Causes of cellulitis, perichondritis, and chondritis |
trauma (usually penetrating) piercings ear surgery (iatrogenic - treatment induced) underlying conditions (e.g. diabetes, immunosuppression)
Urgent referral - antibiotic treatment, incision and drainage for abscess
CHL possible when it involves entire ear or closes up the EAM
|
|
|
Susceptibility factors of weather related injuries |
malnutrition (need to be healthy to fight off infection/produce appropriate response) dehydration over-activity or under-activity prolonged exposure poor hygiene |
|
|
Degrees of sunburn |
1st degree: superficial - red, tender, slightly swollen. No referral needed (heals in 1 week) 2nd degree: superficial - very red, swollen 3rd degree: midlevel - sever blisters, peeling skin, nerve damage (no pain) 4th degree: deep - death of soft tissue, muscle, cartilage, bone |
|
|
Weather related injuries - effects on hearing |
ear swells secondary infection physical damage to pinna tympanic membrane involvement |
|
|
Seborrheic dermatitis |

Inflammatory skin disorder eczema like condition scaly, flaky, itchy, and red skin affects sebaceous gland (sweat and wax producing glands e.g. ear canal) rich areas may affect postauricular regions and EAC - if it collects enough it will cause CHL |
|
|
Actinic keratosis |

Pre-malignant lesion caused by sun exposure thick, crusty patches of skin can progress to SCC early removal recommended (surgery, laser, liquid nitrogen) can lead to squamous cell carcinoma |
|
|
Cutaneous horn |

Conical projection above skin surface composed of compacted keratin base may be malignant - requires surgical excision |
|
|
Staphylococcal dermatitis |

Bacterial skin infection caused by staph aureus usually associated with hearing aid molds and poor hygiene |
|
|
Risks of skin cancer |
sun exposure (UV) skin type immunisuppression chronic inflammation genetic predisposition |
|
|
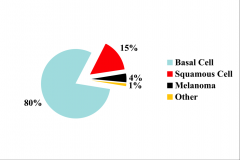
Types of skin cancer - % |
|
|
|
Basal cell carcinoma |

Most common human malignant disease 20% of all cancers in men 10-15% of all cancers in women 85% of all BCC occur in head and neck - due to exposure Raised skin lesion smooth "rolled" pearly translucent border telangiectasia - blood vessels that have burst ulceration and bleeding may be pigmented pruritic |
|
|
Squamous cell carcinoma |

More aggressive than BCC higher incidence of metastasis often a progression from sun-damaged areas (e.g. actinic keratoses) erythematous, crusting, ulcerated (tends to bleed) lesion with granular friable base thick, hyperkeratotic appearance (thick dead skin) Persistent ulceration/bleeding |
|
|
Malignant Melanoma |

Most aggressive type of skin cancer responsible for 75% of deaths caused by skin cancers increasing incidence - especially in young people derived from melanocytes dark pigmented lesion treatment - surgery, chemotherapy, immunotherapy, radiotherapy |
|
|
Features of Melanoma |
Asymmetry Borders (irregular) Colour (variegated) Diameter Evolving over time
great tendency to metastasize |
|
|
Cerumen |
Cerumen which obscures the TM should be removed Ear drops (mineral oil or baby oil, acetic acid, cerumenex softens the wax and it will come out - TM must be intact) Irrigation/flushing (TM must be intact) |
|
|
Aural Atresia/Stenosis |
Atresia - complete absence of EAC (no connection to middle ear) Stenosis - narrowing of EAC Congenital cause of CHL |
|
|
Otomycosis |
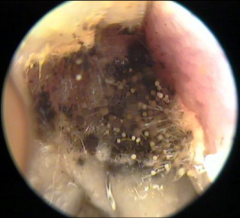
Fungal infection of the EAC Fungal elements visible Aspergillus fumigatus, Aspergillus niger, Candida albicans are most common forms Features wet feeling in the ear Pruritis (itching) deep within the ear Dull pain or discomfort hearing difficulties (CHL) may present similar to otitis externa (fungal vs bacteria) Treatment Difficult to manage refer to ENT for thorough cleaning and drying (microdebridement) application of topical antifungals |
|
|
Oral Candidiasis |
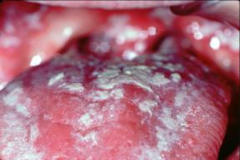
Fungal infection can happen anywhere in the head and neck - moist areas Repeated fungal infection - indicates immunosuppression |
|
|
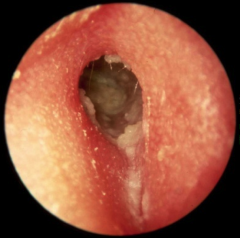
Otitis Externa |
Inflammation/infection of the EAC Bacteria induced most common condition that affects the EAC Acute and chronic types Ear canal skin is injured/abraded by trauma and/or prolonged water or humidity exposure, normal protective wax layer is disrupted and basic (non acidic) environment is formed. Bacteria flourish in basic environment |
|
|
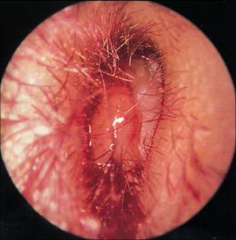
Acute Otitis Externa |

Acute infection of the EAC by Pseudomonas auriginosa Causes spontaneous /idiopathic (don't know cause) local trauma frequent swimming chronic OE - acute flare ups on top of acute Symptoms Otalgia with ear movement Otorrhea Pruritis EAC swelling and collection of debris/discharge CHL Treatment Analgesics antibiotic/anti-inflammatory drops aural toilet (ENT) counselling for prevention - no qtips and ear plugs for swimming
|
|
|
Chronic Otitis Externa |
Chronic inflammatory process persistant symptoms (clinical features for > 2 months) - unrelenting pruritis, mild discomfort, dryness, swollen, narrow ear canal, inflammed, watery debris Bacterial, fungal, dermatological, and chronic/water etiologies Treatment similar to acute OE topical antibiotics/steroids frequent cleaning rarely, surgical treatment (canalplasty) |
|
|
Necrotizing Otitis Externa |
Aka malignant external otitis Infection of the temporal bone - osteomyelitis (bone infection) Mostly affects elderly with diabetes - immunosuppressed Often preceded by EAC trauma or OE Features severe otalgia (pain) otorrhea (drainage) granulation tissue (fleshy tissue in ear canal) cranial nerve weakness (facial palsy) intracranial complications may be lethal Management Urgent referral topical antibiootics aural toilet prolonged IV antibiotics surgical debridement
|
|
|
Foreign Bodies |
Often gets stuck in isthmus - bugs, kids stick things in
|
|
|
Exostosis |
Bony growth in EAC location - frequently bilateral, arises near the annulus/TM Radiographic appearance - broad base, solid associated with prolonged cold water exposure (surfers) May cause CHL
|
|
|
Osteoma |

Bony growths in the EC (solitary) location - unilateral, lateral EAC - not as close to TM as exostosis Radiographic appearance - not solid, pedunculated (on a stalk) No association with cold water exposure Typically no CHL |
|
|
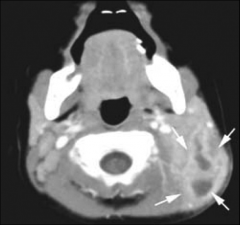
Malignant Lesions of EAC |
May arise within EAC or extend from auricle Radiographic appearance - destruction of bony cortex Most common types - basal cell carcinoma, squamous cell carcinoma, glandular carcinoma skin is so close to bone so skin cancer can travel quickly to bone |
|
|
Keratosis Obturans |

Desquamated keratin accumulation in the EAC Location - involves entire EAC Radiographic appearance - expansion of bony EAC, soft tissue density occupies EAC History of sinusitis of bronchiesctasis - dead skin debris collecting in the ear canal, lots of build up can cause CHL
|
|
|
Cholesteatoma of EAC |
Collection of keratinizing squamous epithelium in EAC Demonstrates independent growth and destruction of local structures Radiographic appearance - destruction of adjacent bone Clinical exam may demonstrate pain, drainage and bleeding Can also occur in mastoid bone
|
|
|
Otitis Media |
inflammation of the middle ear - most common infection in childhood, reason for paediatrician visits and reason for antibiotic use |
|
|
Acute Otitis Media |
Otitis media with middle ear effusion |
|
|
Otitis Media with Effusion (chronic) AKA Secretory OM, chronic serous OM and glue ear |
Middle ear effusion (fluid) without signs or clinical features of acute inflammation/ infection |
|
|
Peak incidence of Otitis Media |
Between 6-18 months - 50% of children by age of 1 yr - by 3 years > 85% of children have had 1 episode |
|
|
Chronic Suppurative Otitis Media |
Chronic purulent otorrhea (thick whitish fluid) through a permanent TM perforation or due to cholesteatoma |
|
|
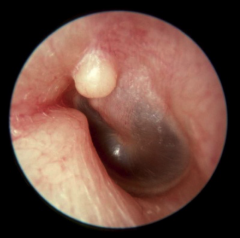
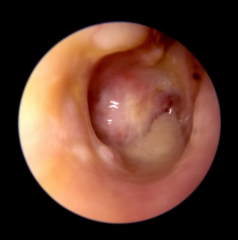
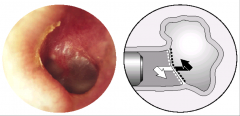
Symptoms of AOM |
Acute onset of symptoms Acute inflammation (fever, pain, otalgia) Redness (erythema) Bulging TM (being pushed out laterally but liquid) Pus in middle ear space Pars flaccida fills up, making superior portion of malleus disappear, pars tens fills up making the distal portion of the malleus disappear Epithelial crusts on TM - sign of recent AOM |
|
|
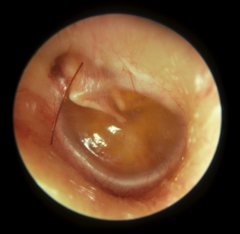
Symptoms of OME |
yellowish hue malleus more pronounced (negative pressure sucking TM in) |
|
|
Definition of Acute, Subacute and Chronic OM |
Acute OM <3 week course Subacute OM 3 weeks to 3 months Chronic OM > 3 months |
|
|
Pathophysiology of OM |
Upper respiratory infection (cold, congestion, flu) Inflammation of nose and ET ET dysfunction/obstruction Negative middle ear pressure Middle ear secretions |
|
|
Muscles of ET |
Tensor veli palatini - tenses the palate Levator veli palatini - lifts tha palate Salpingopharyngeus |
|
|
Functions of the ET |
Pressure regulation of middle ear protection from nasopharyngeal sounds and secretions clearance of middle ear secretions - mucociliary lining
ET connects middle ear to nasopharynx, ciliated respiratory epithelium drain secretions to back of throat ET is usually collapsed. Opening typically happens when swallowing/ yawning and involves cartilaginous portion and palatal muscle function |
|
|
ET - differences between children and adults |
Children - longer bony portion/shorter cartilaginous portion - 10 degree angle from horizontal - small nasopharyngeal orifice in infants (4-5 mm), blocked more readily - less mature muscle - age 2-4 ET becomes easier to open
Adults - anterior 2/3 cartilage/posterior 1/3 bony - 45 degree angle from horizontal - large nasopharyngeal orifice (8-9mm) - more mature muscles |
|
|
Patulous ET |
ET tube opens too easily |
|
|
ETD/OM |
ET does not open easily |
|
|
What do kids present with when they have AOM |
Tugging at ears (with other features can be linked to AOM) putting fingers in ears pain Preceded by cold or URI |
|
|
URI features |
Local - otalgia, otorrhea, hearing loss, ear tugging systemic - fever, malaise, irritability |
|
|
Treatment of AOM |
Antibiotics - refer to GP or pediatrician |
|
|
Bacteria causing AOM |
Streptococcus pneumoniae Haemophilus influenza Moraxella catarrhalis |
|
|
Viral infections (URI) that often precede AOM |
Rhinovirus RSV Influenza Adenovirus Parainfluenza |
|
|
Antibiotics and AOM |
Upper respiratory viral infection reduced immune response increased risk of AOM increased in antibiotic resistance increased antibiotic use |
|
|
Risk factors of AOM |
Daycare First Nations Winter months Bottle feeding Smoke exposure Lower socioeconomic status Allergies Craniofacial disorders (cleft palate) Immune deficiency Reflux disease Nasal obstruction (adenoid hypertrophy) |
|
|
AOM epidemiology |
Peak incidence in first 2 years of life m > f |
|
|
Vaccines - effectiveness for AOM |
Overall 7% reduction in AOM incidence - marginal decrease individually but significant reduction in health care burden Very effective against severe infection |
|
|
Symptoms of OME |
Usually asymptomatic (no ear pulling or pain) Associated with - mild discomfort - pressure or fullness, ear popping - CHL - Recurrent AOMs |
|
|
Types of middle ear effusion |
Mucoid - thick, glue-like, no bulging and you can see malleus Serous - think, watery, bubbles, yellowish hue Purulent (thick, pus) seen in AOM and CSOM |
|
|
Treatment for Chronic OME |
Most of the time no treatment is necessary - less than 20% still have OME after 3 months Often self-limiting Can cause CHL in children - language delay and poor school performance |
|
|
Long term effects of OME |
Mixed results on development of cognitive, linguistic, auditive and communicative skills Severe hearing loss produces severe impairments, |
|
|
Medical Treatments for OME |
Antihistamines Decongestants Nasal Steroids Antimicrobials
poor long-term effectiveness Prolonged therapy required |
|
|
Surgical treatments for OME |
Tympanostomy tubes Adenoidectomy - if thought to be a contributing problem |
|
|
Treatment for OME - not at risk children |
Watchful waiting for 3 months of onset or diagnosis Hearing test (audiogram and tympanostomy) if persistent for 3 months (fluid/CHL remaining) or if signifiant HL, language delay or learning problems Re-examine every 3-6 months until resolved, HL identified, or TM shows structural changes
refer for medical/surgical treatment |
|
|
Otitis Media and the mastoid bone - assessment |
Middle ear is connected to mastoid bone, fluid in middle ear space leads to fluid in mastoid bone (continuous space)
CT scan - opacification of middle ear and mastoid |
|
|
Diagnosis of OM |
Clinical history Pneumatic otoscopy - assess colour, position and mobility of TM (look for normal compliance and nothing impeding middle ear space) Audiogram - hearing status Tympanometry - complience |
|
|
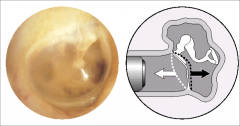
Pneumatic Otoscopy - normal TM normal mobility |
|
|
|
Pneumatic Otoscopy - AOM reduced mobility |
ET closed and middle ear space filled, TM less mobile |
|
|
Pneumatic Otoscopy - OME reduced mobility |
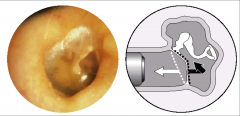
Entire middle ear space may not be filled - TM won't go in as far but will come out typically |
|
|
TM perforation or ear tube - absent mobility |
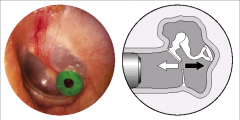
Air goes in and out through tube |
|
|
Audiograms OM |
Pure-tone (usually sound field) - document CHL, SNHL and look for underlying hearing loss Tympanometry - tell you whether there is fluid or not - impedance (compliance, volume, pressure), acoustic reflexes |
|
|
Tympanometry probe parts |
Manometer - varies air pressure against TM and changes ear canal pressure and measures it Speaker - produces a 220Hz probe pure tone Microphone - measures loudness of sound in ear canal which depends on how much is reflected back |
|
|
Tympanometry results for AOM/OME |
Type B |
|
|
Ear tubes AKA tympanostomy tubes or ventilation tubes or pressure equalization tubes Procedure and Function |
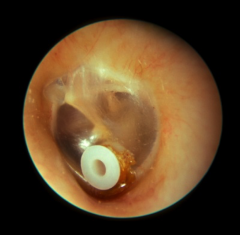
2nd most common surgical procedure in NA Myringotomy - incision in TM Tymanocentesis (collect fluid and send to lab) Function - replacing ET (pressure equalization, middle ear fluid egression) Monitor every 6 months, will heal itself |
|
|
Indication for tubes |
Recurrent AOM Chronic OME (if continuing for >3months, bilateral, causing hearing loss and speech delay) OM or ET dysfunction co-existing with other medical conditions (increases probability of OM) such as craniofacial abnormalities, cleft palate, trisomy 21 TM abnormalities - retraction Complications of OM |
|
|
Complications of ear tubes |
Tymoanosclerosis/myringosclerosis - scaring of TM Persistent Perforation (after tube falls out) Tube otorrhea Tube blockage Granulation tissue - foreign body reaction to tube being in TM for too long. Typically have to remove tissue and tube Cholesteatoma |
|
|
Management Plan for OM |
1st Environmental - breast feeding, control risk factors 2nd Immunization - conjugate pneumococal vaccines, influenza vaccines 3rd Medical therapy - allergy/reflux meds, analgesics, antipyretics, antibiotics 4th Surgical therapy - myringotomy and tubes, adenoidectomy |
|
|
Intracranial complications of OM |
Meningitis Brain abscess (extradural, subdural, cerebral) Sigmoid sinus thrombosis Otitic hydrocephalus |
|
|
Extracranial complications of OM |
Mastoiditis Bezold's abscess Petroud apicitis Facial Paralysis TM Perforation Hearing Loss Labrynthitis |
|
|
Mastoiditis Symtoms |
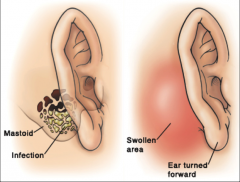
AOM and local inflammatory findings over the mastoid bone - pain - erythema - tenderness - swelling/auricular protrusion - will feel warm
Can be associated with or develop into Bezold's abscess, meningitis, sigmoid sinus thrombosis
|
|
|
Mastoiditis Diagnosis and Treatment |
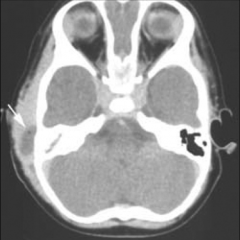
CT - opacified mastoid aircells, middle ear opacification, soft tissue swelling Treatment - IV antibiotics, Tubes (+/-) to drain fluid and collect fluid to be sent to lab |
|
|
Bezold's Abscess |
Spread of infection through mastoid tip to upper neck Presents with AOM and upper neck mass Treatment - IV antibiotics, mastoidectomy, drainage of abscess |
|
|
Petrous Apicitis |
Inflammation of petrous apex portion of temporal bone (infection spread anteriorly) Patients will have classic symptomology - Gradenigo's triad (rtetroorbital pain, otorrhea, CN6 palsy) Treatment - IV antibiotics, temporal bone drill out |
|
|
Facial Nerve Paralysis |
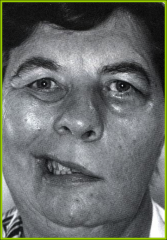
Usually seen with severe AOM in children Possible dehiscent facial nerve in middle ear space (infection eroded bone protecting facial nerve) Good resolution rates Treatment - IV antibiotics, ear tube, ototopical drops Weak side won't move |
|
|
Labyrinthitis |
Inflammation of labyrinth - AOM spreads medially through weak or dehiscent oval window - severe auditory and vestibular loss occurs - pus in cochlea - Nystagmus,, tinnitus, SN hearing loss in addition to CHL and vertigo all appear acutely
Treatment - IV antibiotics but function may not recover |
|
|
Meningitis |
Inflammation of the meninges (dura, arachnoid, pia), if severe enough it can travel into brain (abscess) Symptoms - headache, photophobia, fever, decreased level of consciousness, neck rigidity Diagnosis - CT and LP Mangagement - IV antibiotics (+/- tubes) Audiological follow up |
|
|
Brain Abscess |
Localized collection of pus/infection spread from mastoid/middle ear via venous channels focal neurologic signs and headaches treatment - IV antibiotics, abscess drainage, mastoidectomy |
|
|
Sigmoid Sinus Thrombosis |
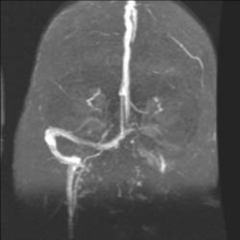
Sigmoid sinus (located posterior to mastoid) Thrombosis = stationary blood clot Symptoms - severe headaches, septicemia (infection in blood stream), picket-fence spiking fevers Clot can spread to other areas Treatments - IV antibiotics, mastoidectomy, anticoagulation |
|
|
Otitic Hydrocephalus |
Increased intracranial pressure From AOM or thrombosis progressive headache can progress to coma, death if drainage inadequate Treatment: reduce ICP (neurosurgery) probes into ventricles to drain fluid |
|
|
Infection control |
Ensure clean and safe environment integrate and comply with infection control regulations wherever you practice Staphylococcus is the most common bacteria found on hearing aids Clean and disinfect equipments, hand hygiene |
|
|
Opportunistic infections |
Infection caused by commonplace microbes in immunocompromised patients (young, old, HIV, other immune dysfunctions) |
|
|
Middle Ear - name parts on diagram |
|
|
|
Tympanic membrane - identify landmarks |
|
|
|
TM 3 layers |
Outer-squamous: epithelial layer Middle-fibrous: structural support of ear drum Inner-mucosa: same as lining in nose/airway |
|
|
Physiology of middle ear and effects that counter impedance |
Transfer of sound energy from low-impedance air to high-impedance cochlear fluid -lever effect: ratio of length of malleus handle and incus structure. 1.3-1.5 times -area effect: area difference between malleus and stapes footplate 20:1 Aerated space Eustacian tube Mastoid space |
|
|
Causes of TM perforation |

Trauma - Qtip, kids stick things in Infection Cholesteatoma Tubes Tympanoclerosis Spontaneous |
|
|
TM perforation - associated problems |
Recurrent infections/otorrhea Chronic irritation - foreign bodies can get into middle ear CHL (reduced immittance mechanism) Reduced impedance
|
|
|
Management of TM perforation |
Monitor (most heal with time) Myringoplasty - patching Tympanoplasty - patching |
|
|
Tympanosclerosis and Myringosclerosis |

Scarring of the TM and middle ear
Scarring of TM only |
|
|
Tympanosclerosis and Myringosclerosis - associated problems |
Both can cause CHL (not common) Rarely SNHL |
|
|
Causes of tympanosclerosis |
Otitis media Tubes TM perforation (anytime the TM is healing scarring can occur) |
|
|
Management of tympanosclerosis |
Usually nothing needs to be done ENT referral for CHL (middle ear exploration) |
|
|
TM Granulation |

Usually related to a foreign body reaction |
|
|
Hemotympanum |

Blood in middle ear space typically caused by trauma |
|
|
Retraction Pockets |

Parts of TM that are retracted or sucked into the middle ear space |
|
|
Middle ear Atelectasis |

Severe retraction/collapse of the TM, thin/weak and stuck to middle ear floor
CHL |
|
|
Bullous Myringitis |
Inflammatory/infectious condition of TM Fluid filled vesicles Sudden onset of severe otalgia Often follows AOM Treat with antibiotics, analgesics and drainage |
|
|
Otosclerosis |
Metabolic bone disease of the otic capsule (inner ear) |
|
|
Otosclerosis Epidemiology |
Congenital but presents later in life typically present in the 2-4th decade of life rarely n children (congenital fixation of stapes) more common in females (2:1) Mostly caucasians 10% of all temporal bones showed histological changes of otosclerosis Becoming less common |
|
|
Otosclerosis Etiology |
Idiopathic Genetic - family history present in 50-70%, autosomal dominant Hormonal - F>M, accelerated during pregnancy Viral - decreasing after measles vaccinations |
|
|
Otosclerosis Pathophysiology |
2 phases - active phase "otospongiosis": osteclasts more active, resorption of bone. Schwartze's sign - redness that you see along middle ear floor indicating vascular tissue in middle ear - mature phase: osteoblasts more active, deposition of new bone
Most common sites of involvement - fissula ante fenestrum (anterior part of footplate) - round window - anterior wall of IAC - where facial and cochlear nerve run - inner ear "cochlear otosclerosis" causes SNHL |
|
|
Otoclerosis Audition |
-Stapes footplate fixation - CHL (beter understanding in noise (percusis of Willis) - inner ear involvement - SNHL -HL progresses from low (early stage) to high frequencies -Low frequency tinnitus - bilateral in 70% of patients |
|
|
Otoclerosis Audiological features |
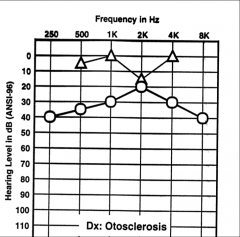
Air bone gap (CHL) Carhart's notch - notch at 2k: air and bone conduction come together to appear as a SNHL (disrupted ossicular resonance/perilymph immobility. Mechanical artifact) Normal discrimination Tympanograms (normal or As - shallow peak) |
|
|
Otosclerosis management |
-Conservative for mild cases - monitor them -Audiological: amplification - Medical: sodium fluoride slows down progression of disease, vitamin D and calcium carbonate - Surgical: bone-anchored hearing aids (BAHA titanium screw in temporal bone, sound processor connected to the screw causing vibrations, sound energy bypasses the external and middle ears), stapedectomy (removal of footplate), stapedotomy (hole made in the footplate) |
|
|
Otosclerosis Amplification and possible problems |
Great option for poor surgical candidates and patients who don't want surgery
Possible problems - canal occlusion effect, sound quality will not be as good, no amplification at night, expensive, cosmetic |
|
|
Bony diseases that can cause CHL |
-malleus head fixation -congenital footplate fixation (Apert) -ossicular discontinuity -osteogenesis imperfecta -paget's disease: increased bone turnover with excessive breakdown leading to weakness, abnormal excessive bone formation, mixed HL (inner ear and ossicular involvement) -osteopetrosis: uniformly increased density of all bones, lack of cortical medullary differentiation, opposite of osteoporosis, CHL -Superior semicircular canal dehiscence: bony defect (opening) of superior semicircular canal, clinical features (autophony, dizziness, CHL, hyperacusis, tullio phenomenon) |
|
|
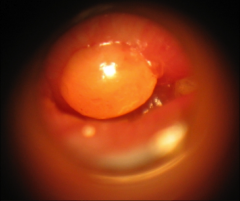
Cholesteatoma |

- a collection of squamous keratin (skin debris) in the middle ear and mastoid (attic/pars flaccida region) - Produces from squamous epithelial cells (typically line ear canal) - exhibits independent growth and locally agressive (destroys structures as it grows)
|
|
|
Cholesteatoma - Keratin physiology |
-EAC and external surface of TM in lined with squamous epithelium - sheds keratin -middle ear and internal surface of TM is lined with respiratory epithelium - no keratin - keratin in the middle ear gets chronically infected and erodes bone |
|
|
Cholesteatoma Epidemiology |
About 5 per 100,000 incidence - decreasing due to good medical treatment High risk population - multiple OMs, ear tubes, cleft palates, trisomy 21 |
|
|
Cholesteatoma Pathophysiology |
Congenital - gradual growth over time, presents early in life. Usually come in for diagnosis around 3-5 yrs Acquired - primary (retraction pocket), secondary (TM perforation). Associated with chronic ETD and recurrent OMs (TM is weakened resulting in retraction pockets or perforation). Presents later in life. |
|
|
Cholesteatoma Levenson criteria for diagnosis |
White mass medial to an intact TM Normal pars flaccida & tensa (no retraction pockets) No history of TM perforation or otorrhea No trauma or surgery |
|
|
Acquired Cholesteatoma |
Primary acquired - chronic ETD - deep retraction pocket (pars flaccid) - collection of keratin within the retraction pocket
Secondary acquired - chronic ETD - recurrent OMs - chronic TM perforation - in-growth of keratin via the TM perforation
|
|
|
Acquired cholesteatoma - other theories |
-metaplasia: transformation of respiratory epithelium to squamous epithelium due to chronic infection. Meta transformation of cell types -implantation: squamous cells implanted into middle ear from trauma or surgery (ear tubes). Keratin debris dragged into middle ear space |
|
|
Cholesteatoma Presentation |
often few signs/symptoms -History- otorrhea (foul smelling), hearing loss, otalgia, aural fullness, dizziness, tinnitus -Past medical history - OMs, TM perforations, trauma, ear surgery Most common presentation involves unilateral chronic otorrhea and hearing loss |
|
|
Cholesteatoma Evaluation |

-Physical exam - otoscopy (pars flaccida crusts and CHL), tuning fork exam, , vestibular exam -audiology - audiogram - imaging - CT scan of temporal bone (determine extent and location of disease, examine ossicles, assess complications associated with disease), MRI (rare) |
|
|
Cholesteatoma Audiological Evaluation |
Mostly CHL Ossicular erosion (CHL) Severity of loss depends on location and extent of disease Labyrinthine fistula (SNHL), vertigo) For large cholesteatomas the AC may be worse than indicated by the hearing test |
|
|
Cholesteatoma Management |
- Refer to ENT -Medical therapy - antibiotic/anti-inflammatory drops to settle down ootorrhea -Surgical therapy- tympanomastoidectomy (gain access to mastoid bone). Goals of surgery: remove all cholesteatoma to obtain a safe and dry ear, restore or maintain functional capacity of the ear, prevent complications) |
|
|
Complications of tympanomastoidectomy |
Complications of surgery - SNHL/dead ear - dizziness/vertigo -facial nerve injury - altered taste (sever chorda tympaninerve) - CSF leak - recurrent or residual disease |
|
|
Complications of Cholesteatoma |
-chronic infection/otorrhea (perf TM) -CHL -dizziness and SNHL with labyrinth fistula (disease moving medially) - facial nerve weakness (disease erodes into facial nerve) - meningitis (disease erodes superiorly into neural tissue) - brain abscesses |
|
|
Familial |
Trait appears in more than one family member |
|
|
Genetic Hearing loss |
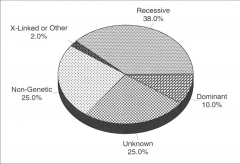
Condition resulting from change or variation in genes, permanent childhood hearing loss due to a genetic cause - inherited - new mutation - always congenital - may not express themselves until later in life (differentiated from acquired disorders) - deafness affects 0.3% - congenital SNHL (50% genetic, 25% environmental, 25% idiopathic) - genetic (75% AR, 20% AD, 5% x-linked) of those 70% non syndromic - classifications no associated abnormalities external ear abnormalities musculoskeletal abnormalities ocular abnormalities integumentary system abnormalities metabolic and renal disorders nervous system disorders cleft and craniofacial disorders |
|
|
New born hearing screenings - Purpose? |
Yoshinaga-Itano Study - if you detect hearing loss early i.e. before 6 months kids get much closer to typical speech/language development norms. - Moral obligation to diagnose early if we can - Age of identification influences - language development - Health (QoL) - Economic (productive life)
Colorado NBHS Study - 291 diagnosed with HL (82% SNHL, 71% bilateral, 47% had 1 or more risk factors- ICU stay, low birth weight, hyperbilirubinemia, family history, maternal infections, syndromes) - overall 92% affected newborns were diagnosed by 5 months of age = effective measure - 50% of congenital SNHL had no history or features that indicated red flag - $25 per child, false positive ($10,000/case) |
|
|
New born hearing screenings - aim and methods? |
Aim is to screen >95% of newborns by age 3 months
Otoacoustic emissions (OAE) - normal cochlea produces low intensity sounds from OHC as they expand and contract which is measured. 3-10% false +ve, cheap and quick
Automated auditory brainstem response (AABR) - different parts of auditory brainstem function as tested using evoked potential generated by click stimuli. 1-3% false +ve, more costly |
|
|
Why do some babies miss NBHS? |
Home birth parental refusal transferred/discharged prior to test certain hospitals |
|
|
How can you pass a NBHS but have hearing loss? |
loss is outside frequencies loss is better than 35dB screening threshold misinterpretation of results by technician equipment malfunction hearing loss occurs after birth auditory neuropathy/dyssynchrony |
|
|
What happens after a failed NBHS? |
Testing repeated prior to leaving hospital referral to audiology in 2-3 months for diagnostic ABR |
|
|
Difficulties in testing children |
Can be uncooperative OAEs and ABRs require quiet, cooperative child After 6 months ABR difficult in natural sleep Behavioural testing success can vary (can overestimate hearing abilities) Developmental delay/ASD/ADD - behavioural testing can be difficult, sedation has risks Auditory neuropathy can be overlooked due to OAEs |
|
|
High Risk Register for Hearing Loss - who should have repeat assessments and who is at high risk for loss? |
- caregiver concern (hearing, speech, language, developmental delay) - family history of permanent childhood HL - NICU >5 days, assisted vent, ototoxic drugs, hyperbilirubinemia - prenatal infections (TORCH) - craniofacial anomalies - physical findings associated with HL syndrome - syndromes with associated HL - neurodegenerative disorders associated with HL - Postnatal infections associated with HL - head trauma - chemotherapy -recurrent or chronic OM (>3months) |
|
|
Genetic HL - No other features |
Primary group that requires NBHS - no obvious anomalies, some develop HL later Some SNHL without other abnormalities is ideopathic Can be mild or unilateral May not be detected until adulthood Early detection is important for development |
|
|
Mild or Unilateral Hearing loss - considerations and impact on speech/language |
Mild -20-40dB permanent SNHL -5-10% of total Aud/SLP caseload - mild bilateral SNHL are much more likey to be offered treatment than unilateral impairments (aids don't consider producing <25dB, provide aids >40dB), therapy, referral)
Unilateral - permanent SNHL in one ear only - 5% of total Aud/SLP caseload
Impact on speech and langauge - phonological awareness - high level language skills (narrated text-less stories) - verbal and non-verbal reasoning - frequency resolution ability (mild loss) - sound localization ability (unilateral loss)
|
|
|
Connexin 26 aka DFNB1 gene/GJB2 gene |
DFNB1 - autosomal recessive mutation in connexin 26 protein - found in chromosome 13 (typically encodes connexion 26 protein or GJB2 protein, 6 proteins join to form a junction channel between cells allowing them to communicate - how IHC communicate) - many different mutations can cause connexin 26 mutation (35delG 85% deletion of 35th base pair, 167delT 9% thymine deleted, M34T 7% switching) - accounts for up to 50% of AR deafness (25% of genetic, 15% of all) - about 1/40 of NA pop carry a mutation in connexin 26 -bilateral SNHL (usually >40dB) - 40% have severe to profound HL - 2% have mild HL - can be progressive - do well with cochlear implants - best to sequence entire gene, requires genetic counselling
|
|
|
Connexin 30 |
SNHL have only 1 mutation in connexin 26 many found to have mutation i nearby gene (GJB6) which codes for connexin 30 SNHL may result in single connexin 26 mutation +single connexin 30 mutation |
|
|
Auditory Neuropathy |
-impairment of sound transmission from inner ear to brain - mild to profound loss with worse than expected speech discrimination - inconsistent response to sound - familial form = mutation in the Otoferlin gene (DFNB9) - autosomal recessive - no syndromic features /radiologic abnormalities - some benefit from cochlear implants - OHC function intact so present with normal OAE and absent/severely abnormal ABRs |
|
|
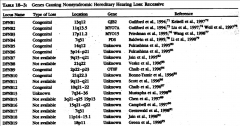
Deafness Genes |
|
|
|
Genetics - basics |
-DNA - deoxyribonucleic acid (adenine-thymine, cytosine-guanine) - 1 gene - made up of 1000 base pairs - Transcription (DNA-RNA - in nucleus), Translation (RNA-Protein - in cytoplasm) - chromosome - packaged bundles of genes, humans have 23 pairs (22 pairs autosomes, 1 pair sex chromosomes). Short arm - p, long arm - q
|
|
|
Genetic hearing loss - chromosomal |
Autosomal - genes on the 22 autosomal chromosomes (1-22) X-linked - involves genes on the sex chromosomes (23) Mitochondrial - only passed on by females
|
|
|
Chromosomal Abnormalities |
extra or missing copies of chromosomes (0.4% of live births) - extra copy of chromosome (trims 21, 18, 13) - deleted copy of chromosome (monosomy 13) - portions of chromosomes rearranged (deletion, duplication, translocation, inversion)
|
|
|
Autosomal recessive |
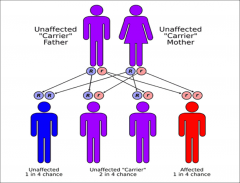
-Need 2 copies of affected gene to express trait, not every generation is affected - 35-40% of all congenital hearing loss - most common pattern of of genetic hearing loss - for offspring to have disorder with parents have to be carriers - 1 in 4 risk |
|
|
Autosomal dominant |

- only need 1 copy of gene for it to be expressed - every generation is affected - 10% of all congenital hearing loss - dominant genes can lack penetrance or show variable expressivity 1 in 2 risk |
|
|
X linked recessive |
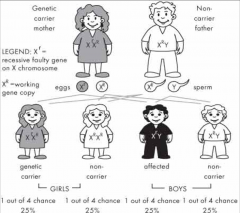
- Mostly recessive, can be dominant (females more likely to suffer from dominant disorders) - transmitted on X chromosome - fully expressed in males (half affected) - females are carriers (half will be carriers) |
|
|
Mitochondrial hearing loss |
MELAS (mitochondirla encephalopathy lactic acidosis stroke) Kearns-Sayre Syndrome (KSS) - all mitochondria inherited from mother, mitochondrial DNA is passed on without division or recombination ( can have spontaneous mutation). Passed on to all children, females pass it on, males are affected but their children are not |