Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
108 Cards in this Set
- Front
- Back
|
Glomerular Structures That are targeted
|
1. afferent arteriole; humoral, immune, thrombotic, pressure...
2. efferent arteriole 3. GBM; thich, thin, deposits 4. Mesangial cell and matrix; expansion, deposits 5. Endothelial cells; hypertrophy, proliferation, atrophy, necrosis 6. Epithelial Cell- visceral and parietal |
|
|
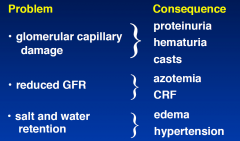
Consequences of Glomerular Disease
|
- red. GFR
- salt and water retention - hypertension - active urinary sediment - proteinuria |
|
|
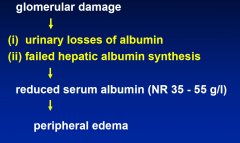
Nephrotic Syndrome
|
1. proteinuria >3.5g/day
2. hypoproteinemia 3. edema - lyperlipidemia - dec. GFR - thromboembolic events - high ESR, infection |
|
|
Nephritic Syndrome
|
- hematuria
- proteinuria - hypertension - renal failure |
|
|
Crescentric Glomerulonephritis
|
- nephritis with rapidly progressive renal failure
|
|
|
Immunofluroscents
|
mesangial vs capillary wall
granular vs linear linear= Good Pastures |
|
|
Light Microscope
|
proliferative vs exudative
endocapillary vs extracapillary global vs segmental diffuse vs focal special stains |
|
|
Electron Micrscope
|
mesangium
GBM endothelial and epithelial cells EDD |
|
|
1o Glomerulonephritis
|
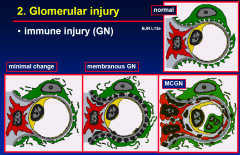
minimal change disease
focal sclerosing GN IgA disease membranous GN crecentic GN post-infectious GN |
|
|
2o GN
|
SLE
vasculitis |
|
|
Misc. GN
|
DM
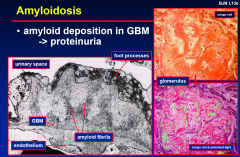
dysproteinaemias (eg amyloid) HT - benign & malignant tubulointerstitial disease |
|
|
Minimal Change Disease
|
nephrotic syndrome
- Tc ? - minimal change on LM, loss of podcyte foot processes on EM Minimal change disease Treatment • empirical prednisolone • cyclophosphamide / CsA for relapse BJN L13e Nephrotic syndrome • childhood 90% (peak 2-4 y.o., males) • adults 15-25% Characteristics • selective proteinuria / nephrotic syndrome • benign urine sediment, normal S. creatinine |
|
|
Focal Sclerosing GN
|
nephrotic syndrome
- microscopic haematuria - CRF |
|
|
Membranous GN
|
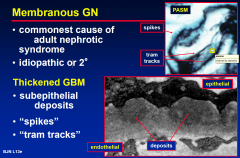
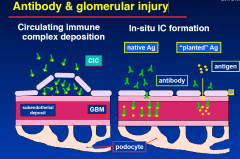
immune complex
tumours SLE drugs- penicillamine, gold - infections- Hep B CRF |
|
|
IgA Disease
|
abnormal IgA regulation
? in response to envirnomental Ag CAUSES microscopic haematuria LEADING to CRF |
|
|
Postinfectious GN
|
NEPHRITIC syndrome
Ab vs Microbial Products |
|
|
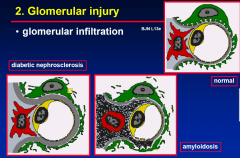
Diabetic Glomerulopathy
|
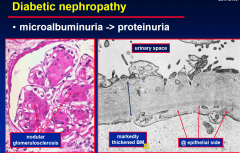
hyperglycaemia
HT microalbuminuria proteinuria CRF |
|
|
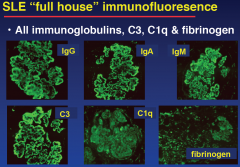
SLE
|
EM only
Ab vs DNA diffuse proliferative membranous NEPHRITIC diffuse proliferative |
|
|
Proteinuria Definitions
|
>0.15g/d
|
|
|
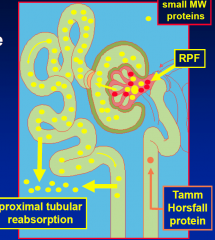
Tamm Horsfall Protein
|
added into the urine from the tubules
|
|
|
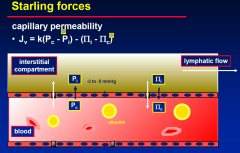
Effects of DEC. Glomerular permeability
- clinically |
|
|
|
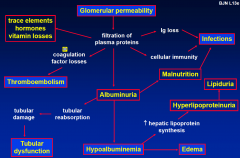
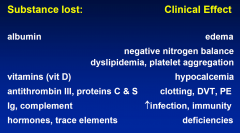
Urinary Losses and their effects
|
|
|
|
Glomerular Injury
- IMMUNE |
|
|
|
Glomerular Injury
- INFLITRATION |
|
|
|
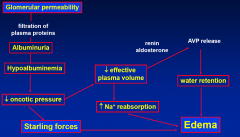
Hypoalbuminemia
|
|
|
|
Oedema
|
|
|
|
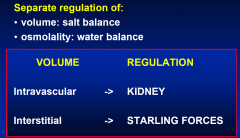
Starlings Forces
|
|
|
|
Edema (underfill hypothesis)
|
|
|
|
DDx Oedema of renal and cardiovascular origin
|
renal is everywhere
CV is mainly in the legs |
|
|
Pitting edema Causes
|
Renal disease:
• nephrotic syndrome • renal failure Other causes: • CCF • liver disease • hypoalbuminemia • venous obstruction |
|
|
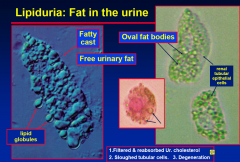
Lipiduria: Fat in the urine
|
|
|
|
Causes of proteinuria
|
1. Glomerulonephritis
• membranous GN • FSGS • minimal change nephropathy • mesangiocapillary (MCGN) 2. Other • diabetic nephropathy • hypertension • amyloid, chronic renal failure |
|
|
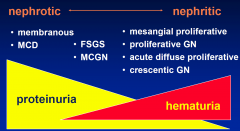
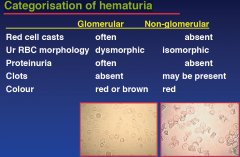
GN & urine sediment
- nephritic vs nephrotic |
|
|
|
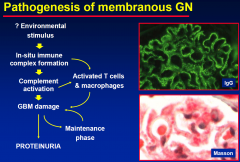
Pathogenesis of membranous GN
|
|
|
|
Causes of membranous GN
|
Causes of membranous GN
1. Idiopathic 2. Secondary • Neoplasia (lung, colon) • SLE • RA, penicillamine, gold therapy • Hep B, Hep C, syphilis • sarcoid, schistosomiasis (rare) |
|
|
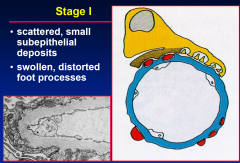
Stage I M-GN
|
|
|
|
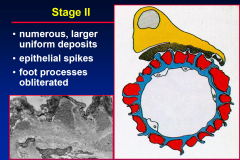
Stage 2 M-GN
|
|
|
|
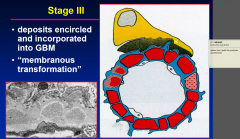
Stage 3 M-GN
|
spikes upset the podcytes and proteinuria starts
|
|
|
Stage 4 M-GN
|
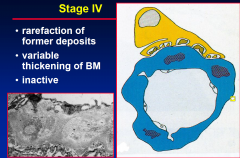
by this stage Immunosuppression Tx is useless
|
|
|
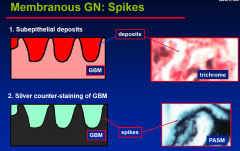
Membranous GN: Spikes
|
|
|
|
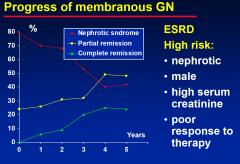
Progress of membranous GN
|
|
|
|
Treatment of Membranous GN
|
Non-nephrotic
• women, young & children (65% remission) • diuretics & wait 6 months BJN L13e Nephrotic or persistent proteinuria • steroids • cyclophosphamide or chlorambucil • ACEI & statins |
|
|
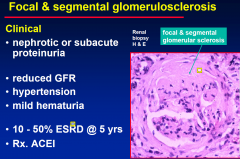
Focal & segmental glomerulosclerosis
|
|
|
|
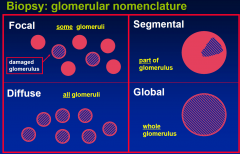
Biopsy: glomerular nomenclature
|
|
|
|
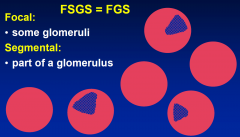
Focal and segmental glomerulosclerosis
NAMING |
|
|
|
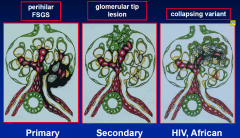
FSGS pathological variants
|
|
|
|
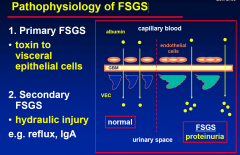
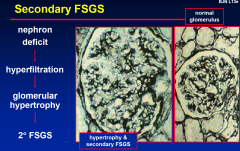
Pathophysiology of FSGS
|
|
|
|
Secondary FSGS
|
|
|
|
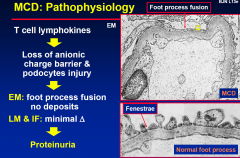
MCD: Pathophysiology
|
|
|
|
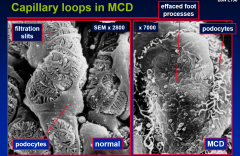
Capillary loops in MCD
|
|
|
|
Diabetic nephropathy
|
|
|
|
Amyloidosis
|
|
|
|
Definition of glomerulonephritis (“nephritis”)
|
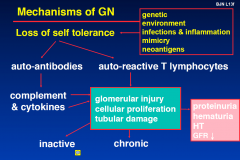
Definition of glomerulonephritis (“nephritis”)
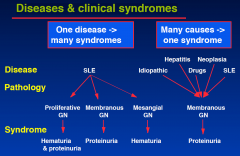
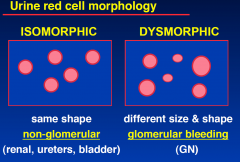
• intra-glomerular inflammation • cellular proliferation -> hematuria (dysmorphic & casts) -> nephritic syndrome (hematuria & proteinuria) Glomerulopathy • non-inflammatory, no cellular proliferation -> proteinuria / nephrotic syndrome |
|
|
Mechanisms of GN
|
|
|
|
Antibody & glomerular injury
|
|
|
|
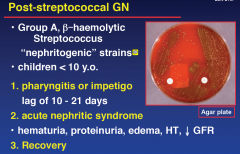
Post-Streptococcal GN
|
|
|
|
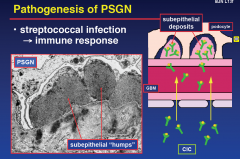
Pathogenesis of PSGN
|
|
|
|
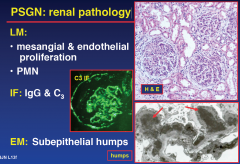
PSGN: renal pathology
|
|
|
|
PSGN:
Dx Course Tx |
Diagnosis
• acute nephritis • ASOT & anti-DNAse B titre • low C3 (+ve RF, CIC, ANF, cryoglobulins) Course • diuresis & recovery 1-3 wks • 5 - 15% mild persistent urinary abnormalities Treatment • diuretics, supportive, ± steroids |
|
|
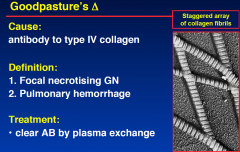
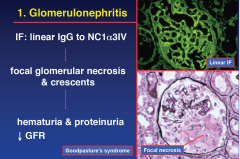
Goodpastureʼs Δ
|
|
|
|
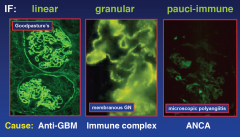
Autoimmunity to BM
|
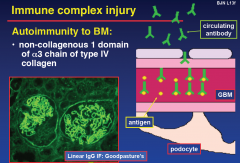
- ONLY linear IgG IF Stain
|
|
|
Goodpasture's
1. Glomerulonephritis |
|
|
|
Goodpasture's
2. Pulmonary Hemorrhage |
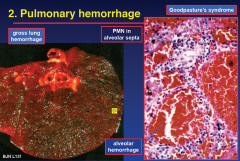
haemorraghe severe enough that the patients die infront of you.
Tx HIGH dose steriods |
|
|
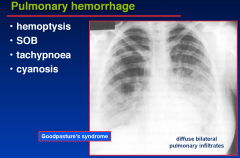
Pulmonary hemorrhage
|
|
|
|
Glomerular immune injury
|
|
|
|
Clinical syndromes of glomerular Δ
|
Asymptomatic proteinuria
Nephrotic syndrome Hematuria (asymptomatic or macroscopic) Acute glomerulonephritis (nephritis ± short term renal failure) Rapidly progressive glomerulonephritis (crescentic GN with renal failure) Chronic glomerulonephritis |
|
|
Diseases & clinical syndromes
|
|
|
|
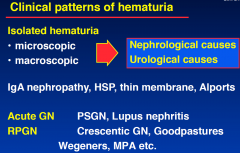
Clinical Patterns of Hematuria
|
|
|
|
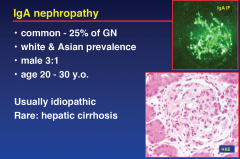
IgA nephropathy
|
|
|
|
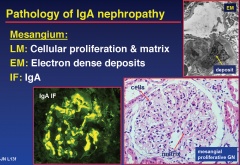
Pathogenesis of IgA nephropathy
|
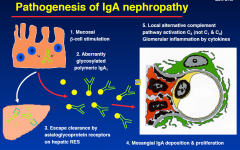
more IgA in corculation and doesnt clear as well causing damage (proliferation of mesangial cells)
|
|
|
Pathology of IgA Nephropathy
- under the microscope |
|
|
|
Clinical IgA Nephropathy
|
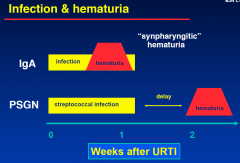
BJN L13f
• recurrent macroscopic hematuria “synpharyngitic” with viral LRTI or gastroenteritis • microscopic (glomerular) hematuria • chronic GN (hematuria ± proteinuria) • hypertension • ↓ renal function • CRF |
|
|
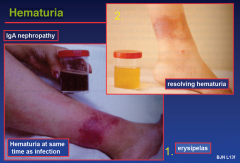
Infections and Hematuria
( 2 cases) |
|
|
|
Hematuria; IgA GN
|
|
|
|
IgA nephropathy
- Dx - Course - Tx |
Diagnosis
• inferred in isolated glomerular hematuria • renal biopsy (if clinically severe) Natural history • usually benign • 10-20% CRF after 20 years (30% after 30yrs) • worse nephrotic, HT, ↑ creatinine, old male Treatment: control BP (no way to contral the IgA primarily) |
|
|
Henoch Schonlein Purpura
|
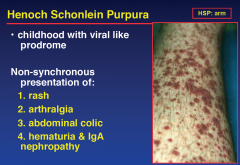
With kidney involvement, there may be a loss of small amounts of blood and protein in the urine, but this usually goes unnoticed; in a small proportion of cases, the kidney involvement proceeds to chronic kidney disease. HSP is often preceded by an infection, such as pharyngitis.
HSP is a systemic vasculitis (inflammation of blood vessels) and is characterized by deposition of immune complexes containing the antibody IgA; the exact cause for this phenomenon is unknown. It usually resolves within several weeks and requires no treatment apart from symptom control, but may relapse in a third of the cases and cause irreversible kidney damage in about one in a hundred cases. |
|
|
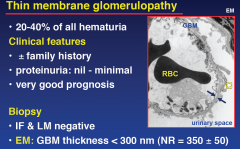
Thin membrane glomerulopathy
|
|
|
|
Rapidly-progressing GN
|
Rapidly-progressing GN
• relentless ↑ S. Cr (subacute or ARF) • active urinary sediment: blood & protein, red-cell casts • normal sized kidneys on US • Bx. crescentic GN • active treatment required Examples: Goodpastures, RPGN, Wegener's granulomatosis, microscopic polyangitis NB: crecentric pattern can be found in more than one disease pattern |
|
|
Cresentic glomerulonephritis
|
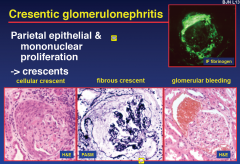
- the crecent squashes the glom. eventually killing it
|
|
|
Vasculitis ;
Systemic Vascular Inflammation |
Clinical features
1. Constitutional symptoms • fever • arthralgia, weight loss, myalgia 2. Localised ischemia • claudication, mesenteric ischemia, bruits 3. Arterial tenderness • e.g. temporal arteritis |
|
|
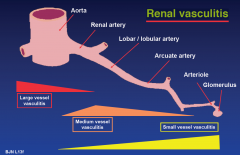
Renal vasculitis
|
|
|
|
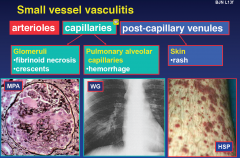
Small vessel vasculitis
|
|
|
|
Classification of small vessel vasculitis
|
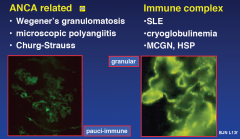
|
|
|
SLE GN
|
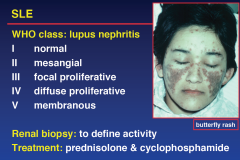
|
|
|
SLE Nephritic or Nephrotic?
|
|
|
|
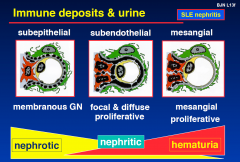
SLE Deposits in...
|
|
|
|
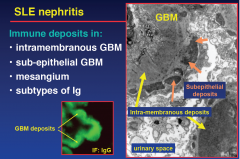
SLE IF
|
|
|
|
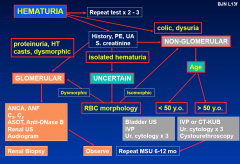
Clinical approach to hematuria
|
Aim:
• distinguish glomerular vs. urological bleeding By: • urine analysis RBC morphology, proteinuria & cytology • imaging (± cystoscopic examination) Isolated hematuria -> exclusion of neoplasia • risk analysis for neoplasia (age, APC intake) • differential diagnosis USUALLY: Haematuria + proteinuria = GN |
|
|
Is it hematuria?
|
A. Is it urinary?
• or contamination from menses, perineal or urethral lesions B. Is it blood? • dipstick • microscopy |
|
|
Other causes of reddish urine
|
Drugs:
• metronidazole, nitrofurantoin, rifampicin, amitryptiline, adriamycin, α methyl-dopa phenytoin, sulphasalazine Aperients: • cascara, senna, anthroquinones Foods: • beetroot, rhubarb |
|
|
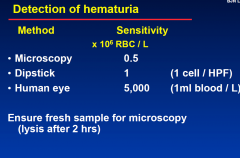
Detection of Haematuria
|
|
|
|
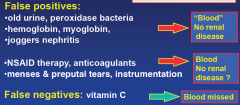
Hematuria by dipstick
False positives |
|
|
|
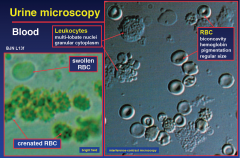
Urine Microscopy
|
|
|
|
Normal Individuals and RBC in urine
|
1 - 2,000,000 RBC / day
< 8,000 RBC / ml 0 - 5 RBC / HPF < 10 RBC x 106 / L Glomerular hematuria (100% dysmorphic) |
|
|
Red cell Morphology
|
|
|
|
Categorisation of hematuria
|
|
|
|
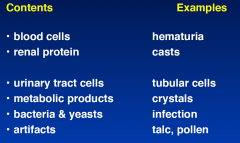
Normal urinary sediment
|
|
|
|
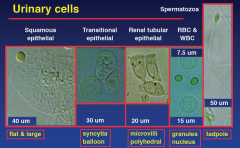
Urinary cells
|
|
|
|
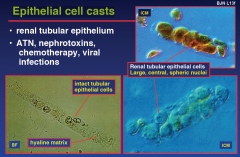
Cellular casts
|
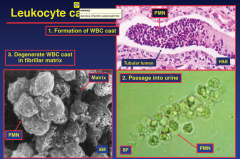
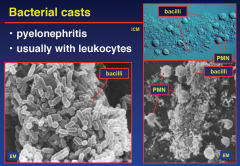
Types:
• red cell cast • white cell cast • bacterial or mixed • epithelial BJN L13f • cellular elements incorporated within matrix formed in distal tubule & collecting ducts • Tamm-Horsfall protein & filtered proteins Types: • red cell cast (ONLY ONES THAT ARE ALWAYS PATHOLOGICAL) • white cell cast • bacterial or mixed • epithelial |
|
|
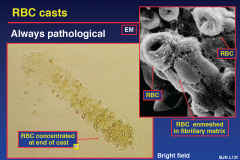
RBC Casts
|
|
|
|
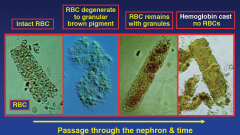
Formation of RBC casts
|
• glomerular damage & urinary bleeding
• addition of Tamm-Horsfall protein • release of red cell cast into urinary stream • modification of cast with passage |
|
|
RBC casts: Stages of degeneration
|
|
|
|
Leukocyte casts
|
|
|
|
Bacterial casts
|
|
|
|
Epithelial cell casts
|
|
|
|
Basic work-up of persistent hematuria
|
• MSU - MC&S, urine RBC morphology
• spot urine protein / creatinine • S. creatinine • sickle cell preparation (African, Indian, Arab) • IVP & bladder-renal U/S or spiral CT (kidneys / prone bladder / KUB) • urine cytology x 3 (may miss grade I TCC) • cysto-urethroscopy (if > 50 y.o.) |
|
|
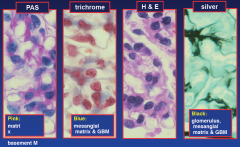
Renal biopsy stains
|
|
|
|
Patterns of immunofluorescence
|
|