![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
142 Cards in this Set
- Front
- Back
|
contagious: |
ability of an infectious disease to spread within a susceptible population by direct or indirect contact |
|
|
infectious: |
disease can be induced by transmission or innoculation of agent/organism |
|
|
infectivity: |
ability to cause infection in a susceptible host (minimum number of infectious particles) |
|
|
pathogenicity: |
ability of agent to induce disease (attack rate: proportion of individuals clinically affected after exposure) |
|
|
virulence: |
ability to induce severe disease or death |
|
|
immunogenicity: |
ability to induce immune response in host that can be protective in case of future exposure |
|
|
what are means of horizontal transfer? |
direct contact, oral, aerosol, vehicle borne, vector borne |
|
|
what are means of vertical transfer? |
trans-ovarial, in utero, colostral |
|
|
endemic: cluster: epidemic: pandemic: |
Endemic: habitual presence of disease within area cluster: a greater than expected group of cases in certain place and time Epidemic: level of disease clearly in excess of expected pandemic: world wide epidemic |
|
|
what is the iceberg concept? |
for one apparent clinically infected animal there are more subclinically infected that remain unseen economic cost of subclinical disease usually exceeds clinical disease- strategic testing to assess prevalence |
|
|
what are four misconceptions due to not understanding the iceberg phenomenon |
considering only clinically ill animals, interpreting absence of clinical cases as absence of disease, presence of infection as indicating agent is cause of disease, decline of clinical cases over time as evidence that interventions were effective |
|
|
what makes up the epidemiologic triad? What are examples of each? |
agent factors (dose, virulence, toxicity), environmental factors (stocking density, movement b/w groups, housing), and host factors (intrinsic- age/genetics or extrinsic- vaccinated/intact/neutered) |
|
|
what is R0? |
mean # of secondary cases a typical case will cause in population with no immunity in absence of interventions basic reproduction number |
|
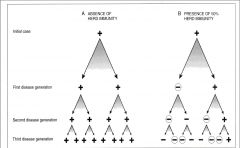
what is Ro of both sides? |
right Ro= 1, will persist in population at stable prevalence left Ro=2, will increase in prevalence |
|
|
what values of Ro indicate the outcome of a disease? What determines R0? |
Ro<1 will die out Ro=1 endemic Ro>1 will spread infectivity of the agent and likelihood of susceptible host encountering agent (amount shedding, stability in environment, number of susceptible animals) |
|
|
what is C? |
C= proportion of population not susceptible 1-C= proportion at risk RoX(1-C)<1 disease can be erradicated |
|
|
why does vaccination not equal immunization? |
approved does not mean efficacious passive immunity, immunocompromised, failure to booster vaccine |
|
|
point source: continuous common source: propagating: |
point source: animals are exposed to the same exposure over a limited, defined period of time (usually one incubation period) continuous common source: exposure to the source is prolonged over an extended period of time propagating: case of disease serves as a source of infection for subsequent cases (serve as a source for later cases) |
|
|
what do the cases vs time look like for point source, continuous common source and propagating? |
point source: rises rapidly, contains definite peak, followed by gradual decline continuous common source: down slope of curve may be very sharp if source removed or gradual if exhausts itself propagating: series of successively larger peaks |
|
|
what are the specific objectives for outbreak investigation? |
determine the cause, identify how exposed, determine extent, take corrective actions, recommend preventive actions |
|
|
what are the steps for outbreak investigation? |
Verify an outbreak is occurring•Gather info from responsible personnel •Establish a case definition•Examine healthy animals•Examine sick animals•Examine dead animals•Consider findings distinguishing casesand others•Develop hypotheses/ rule-outs•Analytical assessments•Reach tentative diagnosis/conclusion•Make recommendations for prevention infuture•Write up/disseminate for others? |
|
|
biosecurity: biocontainment: biological risk management: |
biosecurity: efforts, programs or interventions to exclude introduction (no impact on endemic) biocontainment: measures that reduce the spread of disease on an operation & b/w biological risk management: evaluation of risk and implementation to limit potential dz |
|
|
what are approaches to disease control? |
symptom- specific (moderate sensitivity, poor specificity), agent/disease specific (require microbiological confirmation), route of transmission (easily understood, applicable) |
|
|
what are routes of transmission? |
Aerosol: close contact of respiratory droplet oral: consumption in feed, water or contaminated objects direct contact: may require mucous membranes or wound to enter or may infect skin fomite: inanimate object can transmit vector borne: mechanical or biological |
|
|
what are steps in BRM assessment? |
risk perception (what is a threat), risk assessment (exposures via each route), risk management (risk assessment, short/long term), risk communication (input important, all parties) |
|
|
how can you practice BRM in the veterinary clinic? |
hospital layout, animal flow and housing, people flow, disinfection & maintenance (gross debris first), minimize zoonotic and nosocomial infections (wash, gloves), risk communication (clients and employees) |
|
|
how can you practice BRM in shelter med? |
similar to clinic (mix sick and healthy animals, nosocomial infection & zoonosis), more difficult by financial realities |
|
|
how can you practice BRM in ambulatory practice? |
clean vehicle and use client owned equipment, PPE, wash hands, healthy animals first, sick animals last, risk communication (farmers and employees) |
|
|
direct zoonoses: metazoonoses: cyclozoonoses: saprozoonoses: |
direct: transmitted from infected host to a susceptible host by direct contact, fomite, mechanical vector (no changes of organism) metazoonoses: agent multiples, develops or both in an invertebrate before transmission to a vertebrate host cyclozoonoses: requires more than one vertebrate host but no invertebrate saprozoonoses: requires non-animal development site or reservoir, such as food plants, soil or other organic material |
|
|
direct: indirect: airborne: horizontal: vertical: |
direct: immediate transfer indirect: transmission by intervening factor airborne:dissemination of infectious aerosols to suitable port of entry horizontal: direct or indirect transmission from infected individual to susceptible individual vertical: transmission from one generation to another |
|
|
what is the organism and description of anthrax? what does sporulation require and what is the lethal dose? |
bacillus anthracis- large, gram + non-motile rod, spores, poor nutrients and oxygen lethal dose 2500 to 55000 spores |
|
|
what are the human transmissions for anthrax and what processes do they involve? what about animal transmission? |
cutaneous: occupational (biting flies) inhalation: occupational gastrointestinal: undercooked meat injection usually ingestion of contaminated soil, feed or bone meal, flies other transmission |
|
|
what are animal outbreaks associated with? what are the geographical distributions? |
alkaline soil, drought-flood period in fall/summer ND/SD & SW TX |
|
|
what are the two virulence factors of anthrax? |
capsule: poly D glutamic acid exotoxins: protective antigen (binding sites for factors), lethal factor (macrophage lysis), edema factor (adenylate cyclase) |
|
|
what are the three forms of illness caused by anthrax? |
peracute: ruminants, rapid onset, sudden death, bloody discharge, incomplete rigor acute: ruminants and equine, 1-3days, bleed from orfaces/ internal bleeding, abortions subacute-chronic: swine dogs cats, pharyngeal and lingual edema, ventral edema, asphyxiation |
|
|
how does anthrax present in equine and swine patients? |
Equine: ingestion- death in 48hr, colic insect bites: hot, painful, spreads= death Swine: sudden death w/o symptoms, pharyngeal edema= asphxiation, ingestion of spores |
|
|
what is the diagnosis and treatment of anthrax? Is there a prevention? |
DO NOT OPEN CARCASS, sample peripheral blood (bandage and disinfect), penicillin and tetracyclines REPORTABLE sterne strain : live nonencapsulated spore vaccine, immunity in 7-10 days |
|
|
when should anthrax be high on differential list? |
high mortality rate in group of herbivores, sudden death with unclotted blood from orifices, localized edema |
|
|
what are the three forms of anthrax in humans? |
cutaneous- 3-5 days, pruritic papule, necrotic ulcer, central black eschar, severe edema inhalation- 1-7days, initially nonspecific, second phase: severe respiratoy distress, mediastinal widening, die 24-36hrs, 75-90% fatality GI- severe gastroenteritis, 2-5days, 25-75% fatality |
|
|
how do you diagnose and treat anthrax in humans? |
isolate in blood, skin or respiratory secretions serology- rapid ELISA, 2004 nasal swabs as a screening tool penicillin is the drug of choice, ciprofloxacin if resistant |
|
|
what are prevention measures for anthrax in humans? |
human vaccine- wool mill workers, vets, lab workers, military wear protective clothing, quarantine area, REPORT burn or bury carcass, decontaminate (quicklime for soil, 1:10 bleach) |
|
|
what do TSE's have in common? |
caused by infectious protein particle: altered endogenous protein and altered 3D conformation transmissible: oral transmission, intracerebral inoculation, blood transfusions spongiform lesions encephalopathies NOT encephalitides: no inflammation lymphoreticular system plays role genetic component |
|
|
what are the differences between TSEs |
distribution of infectivity: scrapie widely distributed, CWD less widespread, BSE narrow tissue distribution species barrier: ability to cause neurologic dz, pathognomonic lesions, detect PrPres, high for CWD and scrapie, minimal for BSE strains will cause different lesions, digestion and blotting patterns and clinical features depending on species |
|
|
what are barriers in place to prevent BSE in the US? |
prevent dz from entering the country, prevent infectious material from entering cattle feed (amplification), detect infected cattle at slaughter, prevent potentially infectious material from entering food supply, stop eating beef |
|
|
what animals are considered high risk for BSE surveillance program? |
adult animals with neurological signs, downer cows, rabies-negative cattle, cattle dying on farms |
|
|
what steps are taken to prevent infectious material from entering the food supple? |
spinal cord can't be used in Advanced meat recovery (AMR), downer cattle banned from food supply, carcass held until results recieved, cannot use spinal cord, skull, etc in cattle >30mo, or distal ileum and tonsils in all cattle |
|
|
what is the rendering rule and why was it made? what are issues with the rule? |
exclude tissues from feeds "cattle material prohibited from animal feed" extend people food restriction to animal feed costly and encourages improper disposal of carcasses (scavengers increase risk of spread) |
|
|
what is brucellosis? describe the morphology |
chronic dz involving the reproductive tract of animals resulting in abortion/infertility gram negative, aerobic coccobacilli, facultative intracellular |
|
|
brucella abortus brucella suis brucella melitensis brucella canis brucella ovis |
brucella abortus: cattle abortions brucella suis: swine abortions brucella melitensis: sheep and goats abortion brucella canis: dogs, abortion epididymitis brucella ovis: ram epididymitis rarely abortion |
|
|
what is the pathogenesis of brucella? |
enter through mucosa, replicate in lymphnodes, survive in macrophages (spread to other tissues- hemolymphatic, repro, udder, joints and bursa) |
|
|
which of brucella abortus brucella suis brucella melitensis brucella canis and brucella ovis are zoonotic and what is the severity? |
Zoonotic, most to least virulent: B. melitensis>> Brucella suis, B. abortus>>>>> B. canis not zoonotic: B. ovis |
|
|
what is the current cooperative program for brucellosis eradication? |
surveillance (agglutination card), vaccination (RB51- attenuated strain, no reactive Abs for agglutination), indemity: pay for reactors |
|
|
what is the US barrier to eradication? |
endemic in Yellow stone national park wildlife and mexico, MT, ID, WY and TX free last 1-5yrs |
|
|
how does WHO view the need for a human brucellosis vaccine? |
most widespread of all zoonoses, toll on people and animal industry, development of human vaccine, animal control and surveillance as high priority |
|
|
what are the signs of brucellosis in humans? |
acute or insidious onset of fever, night sweats, undue fatigue, anorexia, weight loss, headache, and arthralgia |
|
|
what are long term affects of human brucellosis? |
osteoarthritis, synovitis, endocarditis, CNS and genitourinary relapse common- long term antibiotic treatment |
|
|
what is the importance of unpasturized milk? |
brucella transmitted through ingestion |
|
|
what are signs of humans with leptospirosis? |
2-29day incubation, biphasic Acute: fever, myalgia, headache, chills, diarrhea chronic: all signs above, uveitis, renal or hepatic failure, pulmonary hemorrhage (weil's dz) |
|
|
how is leptospirosis transmitted to humans and animals? |
direct: MM or abraded skin contact with urine, transplacental or venereal indirect: contaminated water humans: contaminated food or water, aerosol, skin abrasions |
|
|
what are two important serovars in cattle and one in swine? |
L. pomona and hardjo L bratslavia - pigs |
|
|
how do you treat leptospirosis in humans and animals? |
dogs: penicillin followed by doxycycline for 2 wks LA: tetracyclines humans: tetracycline, doxycycline, amoxicillin |
|
|
what are the variation in vaccines between people and animals? |
killed whole cell bacterins cattle: 5 way (C,G,H,I,P) dogs: 2 way (C,I) 4 way (G&p) no vaccine available for people except in china |
|
|
what are occupations/situations that increase risk of dz? |
farmers, mine workers, sewer workers, slaughterhouse workers, vets, fish handlers, military, slums (rats/poor hygiene) |
|
|
what is the human and bovine etiologic agents for tuberculosis? |
Mycobacterium tuberculosis: human mycobacterium bovis mycobacterium avium: humans with AIDS |
|
|
where is TB globally? in US? |
developing countries, texas, new mexico, california, minnesota, michigan |
|
|
what are route of transmission for animals, humans and between both? |
Animals: aerosol droplets from people/animals (inhaled- housed cattle and pasture cattle), ingestion: pastured cattle, large infective dose required Humans: infected milk, bodily secretions from infected animals |
|
|
what are the regulations in place for animal TB |
caudal fold tuberculin test, comparative cervical test, INFy test, slaughter check: check for TB pathology with trace back |
|
|
what are the necropsy findings of animals infected with TB? |
tuberculous granulomas in any lymphnode, fibrous capsules, lung involvement |
|
|
what is the organ involvement with the 3 zoonotic mycobacteriums? |
m. tb: primary pulmonary involvement M. bovis: tendency for extrapulmonary involvement M. avium: opportunistic mycobacterial agent (AIDS) |
|
|
what are the clinical signs and treatments for TB |
cough fever malasie Tx: rifampin, isoniazid fluoroquinolones |
|
|
what is the etiologic agent, Hosts susceptible, Clinical signs, and Age ofsusceptibility of johne's |
m. avium paratuberculosis, ruminants, chronic diarrhea and weight loss in animals over 2yrs |
|
|
what are similarities b/w johne's and crohns? |
chronic inflammatory bowel dz, may be caused bu M. paratuberculosis, potentially zoonotic |
|
|
what is the etilogical agent for Q fever and the manifestation in animals? |
coxiella burnetii, seen in cattle sheep and goats in found in placenta, milk and other reproductive discharges causes abortions, tick--> ruminant cycle |
|
|
what are the clinical signs in man of Q fever? How is it transmitted and how often is disease apparent/inapparent? |
Acute: febrile illness lasts 7-10 days, vomiting Chronic: endocarditis, hepatitis tick, inhalation, ingestion-- 60% asymptomatic, 2-5% acute LOW DOSE AEROSOLIZED- 1 organism, incubate 3-30d |
|
|
what are the drug choices in humans? is there a vaccine available? |
18-36mo of doxycycline, no vaccine in US |
|
|
what is the etiologic agent of the plague? |
yersinia pestis |
|
|
Which disease form (s) is/are most common? Which disease form most commonly associated with higher mortality? what is the difference between primary and secondary pneumonic? |
bubonic: 80-90% of cases, fever, malaise, chills, headache, bubo (painful lymphnodes) untreated 50-60% mortality septicemic: systemic spread, bubonic plus prostration, shock, DIC, necrosis of extremities, untreated mortality: 100% pneumonic: primary: inhaled, secondary: septicemic form spreads, fever, chills, headache, respiratory distress, hemoptysis |
|
|
what are the typical reservoirs and areas of geographical significance? |
southwest: N NM, S CO, N AZ, Cali rock and ground squirrels, prairie dogs, mice, voles |
|
|
what are transmissions and drugs used for tx: |
flea bite, direct contact, aerosol aminoglycosides, doxy/tetra, chloramphenicol NOT penicillins/cephalosporins |
|
|
Describe some aspects of the disease in wildlife. Know the two epidemiologic cycles. What is the chief US vector of plague? |
most important vector: oropsylla montana, asia africa SA: xenopsylla cheopis sylvatic (wild- greatest human threat): enzootic- slow death rate, changes host= large die offs (epizootic) urban (domestic): rapid die offs |
|
|
Describe the animal species susceptibilities (or lack thereof), clinical presentations, etc. Know some key clinical signs of animal plague. |
serologically positive: bears, bobcats, badgers, fox, skunks rodents: most die off farm animals and dogs: resistant to dz cats: severe illness and die, transmit to humans via fleas, bite, scratch, pneumonic |
|
|
what is the etiological organism for tularemia? what are the different biovars and their reservoirs? |
francisella tularensis A: more virulent, NA, rabbits, squirrels, ticks B: less virulent, Eurasia NA, muskrats, mice, rats |
|
|
what are the common transmissions to man? the infectious dose? |
ingestion (large infectious dose), inhalation (small infectious dose), direct (skinning/necropsy) |
|
|
where are common foci in the US? |
central US, marthas vineyard (imported rabbits for hunting) |
|
|
what are the 6 clinical syndromes seen? which is most common and which is most fatal? |
ulceroglandular: most common, ulcerative lymphadenopathy glandular: no ulcer, lymphadenopathy (75-80% cases) oculoglandular: conjunctivitis, lymphadenopathy oropharyngeal: pharyngitis, diarrhea, vomitting, tonsil pseudomembrane typhoidal: acute, septicemia pulmonary: inhalation, septicemia 30-60% fatal |
|
|
what is the drug of choice in people? |
streptomycin <1% mortality if treated untreated <8% overall, typhoidal/pneumonic 30-60% |
|
|
what animals is tularemia seen in and what are the signs? |
wildlife: usually found dead, hares easily caught Sheep: lymphadenopathy, fever, dyspnea, diarrhea, rigid gait, outbreaks cats: fever, apathy, ulcerated tongue/palate dogs: fever, ocular/nasal discharge, abscess at site of infection |
|
|
what lesions are found on necropsy for an animal with tularemia? |
gray necrotic foci on lymph nodes , spleen and liver thrombosis and infarcts of small blood vessels, enlarged/discolored spleen and liver |
|
|
what is a metazoonoses and what is an example? |
metazoonoses: require both vertebrates and invertebrates to complete transmission WNV |
|
|
what is the etiological agent for RMSF? What are the regions and vectors? |
rickettsia rickettsii NA, mexico, CA and SA ticks- Dermacentor- east & central US, R. sanguineous in Arizona |
|
|
what are the signs and treatment for RMSF? what can distinguish it from other diseases (erhlichia, lyme)? |
fever, headache, anorexia, vasculitis (rash), kidney failure, CNS (fatal), thrombocytopenia history of tick bite doxycycline vasculitis, petchiae hemorrhage rash erhlichia- leukopenia |
|
|
what are the zoonotic ehrlichia |
ehrlichia chaffeensis E. ewingii Anaplasma phagocytophilum neorickettsia sennetsu E. canis (RARELY) |
|
|
what is the erhlichia that infects monocytes? granulocytes? what are the vectors, geography, and drug choice for both? |
E. chaffeensis: human monocytic erhlichiosis, lone star tick, mississippi & south, doxy E. ewingii/ A. phagocytophilum: human granulocytic erhlichiosis, lone start/ixodes, missouri, NE/ NC US, Doxy |
|
|
what are the signs and symptoms of human erhlichiosis? |
tick bite, elevated liver enzymes, thrombocytopenia, LEUKOPENIA |
|
|
what is the etiologic agent, vector and reservoir for typhus? |
Epidemic: Rickettsia prowazekii, lice are vector, humans and flying squirrels are reservoir endemic: murine typhus, rickettsia typhi, vector- fleas reservoir- rodents |
|
|
what are the clinical signs in man? what is the mortality with and without treatment? |
high fever, chills, headache, cough, severe myalgia (Coma) Rash after one week of onset on upper trunk which spreads to the entire body but face, palms and soles doxycycline, vaccine (not commercially available) 1-20% fatality w/ antibiotics, up to 100% without |
|
|
what is the etiologic agent of cat scratch disease? which type of cat is most likely to be infected? |
bartonella henselae, kitten, stray/shelter, fleas, multicats |
|
|
what are the symptoms in humans? |
immunocompromised: bacillary angiomatosis, bacillary peliosis, bacteremia immunocompetent: benign- papule, fever, lymphadenopathy, fatigue. more severe: liver/spleen, neurologic, lymphatic, skeletal |
|
|
what is bacillary angiomatosis? |
tumor like lesions on skin that are not neoplastic peliosis hepatis: lesions on the liver |
|
|
How frequent are asymptomatic human infections? How severe? To what extent? Are most human symptomatic infections? Immunocompromised? |
??????? |
|
|
what are the signs/symptoms of lyme disease? |
early local: skin is initial target- erythema migrans 7-14d after bite, with fever, myalgia, headache, malaise early disseminated: multiple EM lesions, conjunctivitis, meningitis, encephalitis, (CNVII), AV block, arthralgias involves knees late: mo to yrs after infection, joints or CNS |
|
|
what is erythema migrans? what is the treatment for lyme disease? |
initial target sign rash seen with early lyme dz, penicillins and tetracyclines |
|
|
where is lyme disease predominately seen in the US? what is the vector and etiologic agent? |
northeast, midwest, west ixodes scapularis, burelia burgdorferi white footed mouse reservoir |
|
|
what is chronic disease related to lyme? |
not generally accepted, no medical proof but medicine works (pain management) |
|
|
what is the etiologic agent for psittcosis? what are the two forms of this organism and where are they found? |
chlamydophila psittaci elementary body: infectious, in environment reticulate body: non-infectious |
|
|
in what animals is psittacosis seen in? how is it shed? what are the signs? |
psittacines, gulls, doves, pigeons, turkeys, ducks healthy carriers: intermittent disease: young, crowding anorexia, yellow droppings, sinusitis, nervous signs (ataxia- pigeons, trembling- ducks) ANY LETHARGIC BIRD |
|
|
what is the means of psittacosis transmission to humans |
inhalation: elementary body in droppings or feather dust mouth to beak direct contact (plumage) no person to person |
|
|
what are the clinical signs of psittacosis in humans? how do you confirm dz? |
flu-like, throbocytopenia, encephalitis, jaundice, arthritis, lethargy, epistaxis, hepatitis culture, IgM by MIF |
|
|
what is the treatment? prognosis? |
tetracyclines 1-5% fatality with tx 10-40% w/o tx |
|
|
what makes MRSA resistant? what is the difference between hospital acquired or community acquired MRSA? |
b-lactamase producing strains, alter penicillin binding protein hospital acquired: invasive via hand contact with colonized or infected patients community acquired: skin and soft tissue infection (NASAL, skin, perineal and other mucosal colonization) |
|
|
where was MRSA first isolated? what species has it been found in? |
milk cows with mastitis 1st dogs, cats, horses, sheep, pigs |
|
|
where do small animals acquire MRSA? Horses? which are zoonotic? |
SA likely acquire from owners equine found with both community and hospital isolates transmission b/w horses (foal) and humans reported, none found for dogs to humans PPE |
|
|
what is the common name for dermatophytosis? what are the etiologies and what are their sources? |
ring worm! microsporum canis: cats, dogs M. equinum: horse M. nanum: pigs, soil t. mentagophytes: rodents t. verrucosum: cows, sheep goats |
|
|
what is the transmission, pathogenesis and treatment for dermatophytosis? |
arthroconidia infective, keratolytic and keratophilic, hyphae invade stratum corneum terbinafine, griseofulvin |
|
|
what is the etiologic histoplasmosis? what forms are infective? what kind of zoonosis? |
histoplasma capsulatum, microconidia and mycelial forms saprozoonosis: inhalation from bird or bat droppings |
|
|
what are the five clinical presentations of histoplasmosis? |
1. asymptomatic 2. acute pulmonary histo (pericarditis) 3. chronic pulmonary histo 4. disseminate histoplas 5. mediastinal fibrosis, CNS, broncholithiasis |
|
|
what are the controls and tx for histoplasma? |
immunocompromised: antifungals often not treated b/c asymptomatic tree roosts, spelunking, and recently disturbed soils a risk |
|
|
what is the common name, etiologic agent and transmission of sporotrichosis? |
rose handlers dz, sporothrix schenckii, zoonotic from cats, scratches or abrasions |
|
|
what are the three zoonotic streptococci? what are the clinical signs and transmission? |
streptococcus suis: undercooked pork, occupational exposure, meningitis/sepsis streptococcus iniae: fish and dolphin, immunocompromised people, sepsis, arthritis, endocarditis streptococcus canis: most human occurrences non-zoonotic, elderly men who own dogs (distal leg ulcers and sepsis) |
|
|
what are the veterinary erysipelas? |
erysipelothrix rhusiopathiae: fish handlers dz or diamond skin dz in swine human erysipelas: streptococcus pyogenes erysipeloid: fish handlers dz, cutaneous infection of erysipelothrix rhusiopathiae |
|
|
what is the etiologic agent of cryptosporidium? what is the transmission and from who? |
cryptosporidium parvum aerosol (rare) fecal oral, person<---->animal (holsteins> jerseys) dogs and cats possible but minimally zoonotic lakes pools splash parks, water supplies |
|
|
what are the symptoms of cryptosporidiosis in man? |
profuse, watery diarrhea, 1-12 days acute self limiting gastroenteritis, can be asymptomatic in healthy patients or life threatening in immunosuppressed patient nitazoxanide |
|
|
what is the etiologic agent of toxoplasmosis? Who is the DH and IH? where is infection seen? |
toxoplasma gondii DH: cats, intestinal and extraintestinal IH: warm blooded mammals, extraintestinal only |
|
|
what are the modes of transmission for T gondii? |
fecal oral (sporulated oocyst) consumption of infected tissue (bradyzoites) transplacental |
|
|
what are the clinical signs of toxoplasmosis in humans? what are the affects depending on trimester? what about AIDS |
clinical is rare- france, central america or women of childbearing age congenital infections when infected during pregnancy first: 80% severe second: 30% severe third: 70-90% subclinical AID/immuno: death, encephalitis most common sign |
|
|
what animals are susceptible? |
domestic animals: serve as reservoir, sheep and goats (aborting), hogs, cattle (subclinical) wild animals: source, black bears and WTD marine mammals: encephalitis in sea otters |
|
|
what is the etiologic agent of chagas? what areas is it prevalent? what is the transmission? |
trypanosoma cruzi, south>central>>north america, southern US and Cali triatomine (stercoarian) foodborne in milk, fruits, juices |
|
|
which species are affected by chagas? what are the clinical signs in dogs? |
opossums, armadillos, raccoons, coyotes, rats, mice, cats dogs: acute phase- lymphadenopathy, diarrhea, acute myocarditis in 2-3wks post-infection chronic phase- congestive heart failure, cardiac dilation, sudden death |
|
|
what are the clinical signs and mortality of chagas in humans? treatment? |
acute phase: parasitemic, most adults asymptomatic 5% indeterminate phase: follow resolution of acute, non-parasitemic 5-8%, deaths in children, meningoencephalitis, myocarditis chronic phase: year later, myocarditis, megaesophagus 20-30%, cause for progression unknown |
|
|
what are the two species of taenia, who do they occur in and what is the infective stage? what is the disease concern? |
taenia solium: pig to human (DH or IH), cysticerus, neurocystis sarcosis taenia saginata: cow to human (DH), cysticercus, no dz |
|
|
what are the two species of echinococcus, what is the infective stage, what part does humans play in life cycle and where is it found? who is the DH? |
echinococcus granulosus: hydatid cyst, humans IH found in liver and lungs, dogs DH echinococcus multilocularis: hydatid cyst, humans IH |
|
|
what do the cycst look like for E. granulosus? where is it found in US? what is the treatment for cestodes? |
large, won't fit on slide, diagnosed macroscopically AZ, NM, Utah, Cali praziquantel, pyrantel (horse) albendazole |
|
|
what does disease of cestodes depend on? |
depends on location, size, and invasiveness of larval form |
|
|
what four genus and species of nematodes are zoonotic? |
trichinella spiralis, baylisascaris procyonis, ancylostoma caninum, toxocara spp. |
|
|
what is the disease cause, organism (where in the body is it found?), sources, and control of trichinellosis? |
trichinella spiralis, larvae in muscle, grow and encyst. pork and bear meat, must cook meat thoroughly, cook garbage fed to hogs, improve production practices |
|
|
what are the clinical signs and tx for trichinellosis? |
GI, abdominal pain, larval migration through muscle tissue (periorbital and facial edema, eosinophilia) rarely life threatening steroids and antiparasitics |
|
|
what genus and species cause cutaneous larval migrans? what genus and species cause neural, ocular, visceral? |
hookworms, ancylostoma caninum baylisascaris procyonis and toxocara |
|
|
what is the DH, transmission, and distribution of B procyonis? how long does it take for eggs to become infective? |
DH: raccoons transmission: consumption of eggs common in raccoons and widespread through US require 2-4 to be infectious |
|
|
what are clinical features of humans infected with b. procyonis? what is the treatment? how do you diagnose? what are the risk factors? |
asymptomatic, VLM, OLM, NLM no treatment (antiparasitics), limited tests (biopsy) or clinical signs children, pica, raccoon contact |
|
|
what is the DH for t. canis/cati, transmission, and prevalence? what ascarids are humans an aberrant host for? |
DH dogs/cats, transplacental, transmammary and environmental, 100% puppies toxocara canis/cati, ascaris suum |
|
|
what disease occurs in humans infected with toxocara? |
Larva migrans: VLM, OLM, NLM VLM: liver heart lungs muscle, most mild, eosinophilia (<3yrs age) OLM: inflammation, retinal scarring, vision loss, unilateral, granulamatous lesion near retina NLM: CNS, meningitis, encephalitis |
|
|
what are diagnosis, treatments and control methods for toxocara? |
Ab detection, clinical signs antiparasitics, antiinflammatories treat dogs/cats, hygiene, limit fecal contact |