Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
95 Cards in this Set
- Front
- Back
|
External Ear
What are the three classifications of lacerations of the external ear? |
Simple - skins +/- cartilage
Stellate - blunt trauma or crush injury Avulsion - tear or separation |
|
|
External Ear
What is the management of a hematoma? |
I&D with through-and-through sutures and bolster dressing
Systemic Abx |
|
|
External Ear
What is the incidence of keloids in blacks and Hispanics? |
Up to 30% of blacks and Hispanics
|
|
|
External Ear
What is the tx for contact dermatitis of the external ear? |
Removal of offending agent
Benadryl Topical steroids +/- systemic steroids DDx included cellulitis or herpes zoster oticus |
|
|
External Ear
What the S&Sx at the external ear associated with hypothyroidism? |
Dr, thick skin at the pinna & EAC
Acromegaly Enlarged pinna |
|
|
External Ear
What percentage of pt's with Wegener granulomatosis have associated external ear sx? Sx are similar to what? |
About 3%
Sx similar to perichondritis |
|
|
External Ear
What is the lymphatic drainage of the following external ear anatomy? Lateral pinna & anterior canal wall - Superior and upper posterior pinna - Lobule and floor of external ear canal - |
Lateral pinna & anterior canal wall - ant. auricular nodes
Superior and upper posterior pinna - postauricular nodes Lobule and floor of external ear canal - superficial & deep cervical nodes |
|
|
External Ear
What is the percentage of all external ear skin cancers that are basal cell? |
45% - most common malignancy of the ear
|
|
|
External Ear
What type of skin cancer? "erythematous lesion with raised margins" |
BCC
|
|
|
External Ear
What percent of pt's with systemic psoriasis will have ear involvement? |
18%
|
|
|
External Ear
What is the tx for seborrheic dermatitis or psoriasis affecting the ear? |
Good cleaning with irrigation and drying (hair dryer)
Betamethasone for acute tx 1% hydrocortisone solution or lotion 3% salicylic acid solutions |
|
|
External Ear
Explain keratosis obturans, it's pathology and treament |

Karatosis obturans is a rapid accumulation of keratin debris, which may lead to a plugged external auditory canal. May have painless erosion and expansion of external canal. May be associated with drainage, foul odor and secondary external otitis.
Pathology - chronic inflammation and poor epithelial migration Treatment - frequent cleaning, irrigation; topical 1% hydrocortisone; 3% salicylic acid, betamethasone for acute tx (same tx as seborrheic dermatitis) |
|
|
External Ear
What are osteomas? |

pedunculated bone mass developing along suture lines, tympanosquamous, tympanomastoid, occluding osteoma may require surgical removal.
|
|
|
External Ear
What are exostosis associated with? Tx? |

Associated with cold water exposure.
Lamellar thickening of bone of external ear canal. Commonly involving the anterior and posterior canal wall. May cause canal stenosis, cerumen impaction, or limited exposure of the TM. Tx - canaloplasty, skin graft, meatoplasty |
|
|
External Ear
Describe a hemangioma of the external ear canal Tx? |

Soft, reddish or purple mass of external ear canal pulsating on microscopic examination.
Capillary hamangioma usually involutes in childhood. Cavernous does not involute and may extend to surrounding structures. Tx - aspiration; surgery rarely needed. |
|
|
External Ear
Describe a cholesterol granuloma of the external ear canal. Tx? |

Blue-domed cyst, blue eardrum
Fluid "motor oil" color, often thought to be blood Tx - aspiration; surgery rarely needed. |
|
|
External Ear
What are some causes of secondary canal stenosis or atresia? Tx? |
Recurrent or chronic external otitis, associated with acute anterior tympanomeatal angle, trauma, repeated instrumentation or previous surgery
Early tx - expandable wick and packs, topical Abx and steroids Late tx - excision of fibrosis and epithelium, canaloplasty, thin split-thickness skin graft, and meatoplasty. Prolonged postoperative packing reduces recurrent stenosis. |
|
|
Middle Ear & Mastoid
What percentage of all temporal bone fx are longitudinal? How about transverse? |
Longitudinal - 70-90%
Transverse - 20-30% |
|
|
Middle Ear & Mastoid
Is transverse or longitudinal temporal bone fx associated with a higher risk of facial paralysis? |
transverse
|
|
|
Middle Ear & Mastoid
Is transverse or longitudinal temporal bone fx associated with a higher risk of TM disruption?? |
longitudinal
|
|
|
Middle Ear & Mastoid
Which type of temporal bone fx is associated with CHL and which is associated with SNHL? |
CHL - longitudinal (more likely to disrupt the TM and ossicular chains)
SNHL - transverse (more likely to have otic capsule fx) |
|
|
Middle Ear & Mastoid
Which type of temporal bone fx is more likely to present with bleeding from the external canal? Which is likely to present with hemotympanum? |
Bleeding from the external canal - longitudinal (TM involvement likely)
Hemotympanum - transverse |
|
|
Middle Ear & Mastoid
Patient has a temporal bone fx. A CT is obtained to look at the involvement of what? |
Otic capsule - (20%) - chance of SNHL and facial paralysis
|
|
|
Middle Ear & Mastoid
Penetrating injuries of the TM typically involve and anterior or posterior TM? How about burn injuries? |
Penetrating injuries - typically involve the posterior TM
Burn injuries - anterior TM (blasts & barotrauma typically involve the weakened central drum) |
|
|
Middle Ear & Mastoid
What is the acute tx of a penetrating TM injury? |
prevention of secondary infection - antibiotic pack and drops with water exposure; keep the ear dry; infection adversely affects spontaneous healing
Spontaneous healing usually successful in 78-94%, drum skin margins may be microscopically realigned in the first 24 hours |
|
|
Middle Ear & Mastoid
When would a penetrating TM injury require emergency surgery? What is the tx? |
Usually if the injury involves SNHL and vertigo, suggesting fracture and impaction of the stapes footplate into the vestibule or perilymph fistula
Emergency tx involves sealing the oval window and repairing the TM. Reconstruct the ossicular chain as a secondary procedure depending on residual hearing and bone conduction audiogram Late tx - tympanoplasty (indications are: persistent perforation after 4 months; CHL > 20dB) |
|
|
Middle Ear & Mastoid
What is a potential problem at tympanoplasty that can lead to significant longer term morbidity? |
squamous epithelium in growth onto the medial surface of the drum may extend farther than anticipated = cholesteatoma; may involve the anterior annulus and eustachian tube as well as the ossicular chain.
|
|
|
Middle Ear & Mastoid
What percentage of pt's with Wegener granulomatosis have associated middle ear/mastoid involvement? What are the S&Sx and the pathology? |
19% (remember that external ear was only 3%)
Will see chronic inflammation and granulation tissue formation. CHL, serous otitis media |
|
|
Middle Ear & Mastoid
What are the S&Sx of tuberculosis affecting the middle ear? |
Thickened TM with loss of landmarks, CHL, multiple or total perforation with serous drainage
(spread is hematogenous or lymphatic to temporal bone) |
|
|
Middle Ear & Mastoid
What S&Sx will polyarteritis nodosa cause with middle ear involvement? |
SNHL, sudden HL, facial paralysis
|
|
|
Middle Ear & Mastoid
What S&Sx will sarcoidosis cause with middle ear involvement? |
Facial paralysis, cochlear-vestibular neuropathy
|
|
|
Middle Ear & Mastoid
Van der Hove's syndrome is a subtype of which systemic disease? |
An inherited autosomal dominant subtype of osteogenesis imperfecta
Tx in middle ear involvement: stapedectomy; generally good results |
|
|
Middle Ear & Mastoid
Describe Paget disease in middle ear involvement. What is the pathology? What are findings on CT scan? What is the tx? |
Osteitis deformans; Male:female ratio 4:1. Inherited autosomal dominant. Thickening of the skull. Mixed CHL. Thickening of the ossicles with fixation.
Pathology - vascular, spongy bone, thick or enlarged ossicle, and otic capsule. CT Scan - thickening of cortical bone, ossicles, and otic capsule. Tx - stapedectomy (fragile ossicles and otic capsule), hearing aid |
|
|
Conductive Hearing Loss
What is the incidence of otosclerosis? |
White population - 8-12%, clinical dz - 0.5-2%
Black population - 1%, clinical dz - 0.1% Female:male ratio - 2:1 |
|
|
Conductive Hearing Loss
What percent of pt's with otosclerosis have a FHx of the dz? |
49-58%
|
|
|
Conductive Hearing Loss
What are the early & late phases of otosclerosis pathology? |
Early phase - vascular, spongy bone progressing to fibrosis
Late phase - new bone replaced with sclerotic bone Foci - 67% one, 27% two, 6% three or more Anterior oval window, fistulae, antefenestrum - 70-90% Round window - 30-70% |
|
|
Conductive Hearing Loss
Which virus is associated with otosclerotic foci? |
Measles virus
|
|
|
Conductive Hearing Loss
What is the most common presentation ages in otosclerosis? |
30-50yo
|
|
|
Conductive Hearing Loss
What are the audiometry results in otosclerosis? |
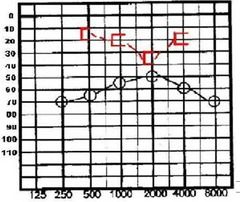
Progressive, low freq, conductive or mixed HL
Maximum conductive component, 60dB Carhart notch, depressed bone threshold around 1000-2000 Hz Word discrimination is good, 70% or better |
|
|
Conductive Hearing Loss
What are the early and late acoustic reflex results in otosclerosis? |
Early - diphasic reflex (occurs even before CHL is detected) - increased compliance at the onset and cessation of the sound stimulus - occurs in 94% with sx of less than 5 yrs, and in 9% greater than 10yrs (40% of normals have a diphasic acoustic reflex)
Late - NO reflex (stapes fixation) |
|
|
Conductive Hearing Loss
What are the Webber and Rinne tuning fork results with otosclerosis? |
Webber - lateralized to affected ear
Rinne - negative - bone > air, masking the opposite ear with unilateral hearing loss |
|
|
Conductive Hearing Loss
What are the air-bone gap dB for the following tuning fork results? Negative 256 Hz Rinne - Negative 512 Hz Rinne - Negative 1024 Hz Rinne - |
Negative 256 Hz Rinne - 15 dB or more
Negative 512 Hz Rinne - 25 dB or more Negative 1024 Hz Rinne - 35 dB or more |
|
|
Conductive Hearing Loss
What are the surgical indications for otosclerosis? |
CHL 20dB or greater
Negative Rinne test, 256 and 512 Hz (good candidate >15-25db loss) Negative Rinne test, 1024 Hz (excellent candidate, >35dB loss) Good bone conduction threshold Speech discrimination 70% or better Stable middle and inner ear Poorer-hearing ear done first |
|
|
Conductive Hearing Loss
What are the age and occupation relative contraindications to otosclerosis? |
Age - child less than 18 yrs of age
Occupation - roofer, acrobat, scuba diver (due to risk of prolonged postoperative vertigo) |
|
|
Conductive Hearing Loss
Are there any medical treatments for autosclerosis? |
Sodium fluoride
Calcium Vitamin D (widely accepted by not FDA approved) Indications for medical tx are cochlear otosclerosis and bone conduction loss greater than 5dB in less than 12 months |
|
|
Conductive Hearing Loss
What is the incidence of perilymph fistula after otosclerosis surgery? |
0.3-2.5%
|
|
|
Conductive Hearing Loss
What is the most common reason for revision stapes surgery in otosclerosis? |
displaced prosthesis (next mc reason is incus necrosis)
|
|
|
Conductive Hearing Loss
What are the causes of vertigo and hearing loss in stapes surgery? |
Suction in the oval window
Excessive manipulation of stapes or prosthesis Long prosthesis Failure to seal oval window Perilymph fistula Disruption of membranous labyrinth Removal of prosthesis Heat from laser |
|
|
Conductive Hearing Loss
Incomplete absorption of Reichert or Meckel's cartilage causes what? |
Fixed malleus or Incus
|
|
|
Conductive Hearing Loss
What does the audiogram look like in a case of fixed malleus or incus? |
Flat conductive hearing loss, 15-20 dB air-bone gap
Congenital - 35-50 dB air-bone gap |
|
|
Conductive Hearing Loss
What is the tx for fixed malleus or incus? |
anterior atticotomy with division of the anterior malleolar ligament and mobilization of the malleus, & tympanoplasty type III.
Transection of malleus neck and anterior malleolar ligament Incus interposition or partial ossicular prosthesis between stapes and malleus handle and drum |
|
|
Conductive Hearing Loss
What is the etiology of ossicular discontinuity? |
Trauma, basilar skull fxt, chronic otitis media, eustachian tube dysfunction, previous surgery
|
|
|
Conductive Hearing Loss
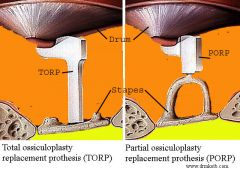
What kind and severity of hearing loss would you expect to see in ossicular discontinuity? What are the tx options? |
CHL of 25-60dB
Tympanoplasty with ossicle interposition or partial ossicular prosthesis (PORP) or total ossicular prosthesis (TORP), repair of the incudostapedial joint-bone cement |
|
|
Conductive Hearing Loss
Describe facial nerve prolapse and what kind and severity of hearing loss can be expected? |
Dehiscent facial nerve impinging on stapes superstructure
Occurs in children (congenital) and adults Flat CHL with 15-25 dB loss (may be 10-20dB loss after successful stapes surgery) |
|
|
Conductive Hearing Loss
Describe congenital cholesteatoma and etiology |
Cholesteatoma developing behind an intact TM with no significant hx of OM
Etiology - epithelial rest cells; sites - anterosuperior quadrant mesotympanum and tympanic membrane adjacent to malleus and posterior mesotympanum |
|
|
Conductive Hearing Loss
What is the pathology of cholesterol granuloma? |
Cyst or fluid within mastoid or petrous apex
May expand into posterior fossa Contains hemosiderin, cholesterol crystals, chronic inflammation Thought to be cause by bleeding or negative pressure; usually develops in previously pneumatized temporal bone |
|
|
Inner Ear Disorders
Meinier's dz (Endolymphaitc hydrops) - what 4 sx? |
HL, vertigo, tinnitus, fullness
|
|
|
Inner Ear Disorders
In Meinier's dz, what are the criteria for vertigo? |
Spontaneous vertigo lasting minutes to hours
Recurrent vertigo- 2 or more episodes lasting >20min Nystagmus with vertigo |
|
|
Inner Ear Disorders
What is the staging of Meniere's dz? |
Stages 0 - VI
Stage 0 - no disability Stage IV - frequent recurrent vertigo greater than 4 weeks per year Stage VI - chronic or incapacitating vertigo |
|
|
Inner Ear Disorders
Describe atypical Meniere's dz |
Incomplete sx complex
Vestibular hydrops - episodic vertigo Cochlear hydrops - fluctuating hearing loss |
|
|
Inner Ear Disorders
Describe Lermoyez Syndrome |
Increasing tinnitis, fullness & HL prior to an attack of vertigo, after which hearing improves
|
|
|
Inner Ear Disorders
Describe Crisis of Tumarkin |
Drop attacks; Otolithic crisis
|
|
|
Inner Ear Disorders
What is the incidence of Meniere's dz? |
In US is 194 per 100,000
Increasing bilateral involvement with length of dz |
|
|
Inner Ear Disorders
What are the medical tx for Meniere's dz? |
Diet: low salt (<2000 mg/d); dietary log to identify sources of salt
Diuretics: HCTZ; carbonic anhydrase inhibitors; acetazolamide Labyrinthine suppressants: dimenhydrinate; meclizine; diazepam (valium); promethazine HCl (phenargan) Middle ear steroid perfusion: decadron or methylprednisolone; variable results for hearing and vertigo relief |
|
|
Inner Ear Disorders
What are some surgical procedures for Meniere's dz? |
Chemical labyrinthectomy - gentamicin profusion of round window
Endolymphatic sac procedures Vestibular nerve resection (hearing preserved) |
|
|
Inner Ear Disorders
List some systemic autoimmune disorders associated with autoimmune inner ear dz |
Polyarteritis nodosa
Wegener granulomatosis SLE Rheumatoid arthritis Ulcerative colitis |
|
|
Inner Ear Disorders
What is Cogan syndrome? |
Interstitial keratitis
Vertigo, bilateral progressive SNHL Hypersensitivity with vasculitis Bilateral symptoms of Meniere's dz |
|
|
Inner Ear Disorders
What is the incidence of idiopathic SSNHL? |
5-20 per 100,000 per yr.
Median age 40-54 yrs Male=female |
|
|
Inner Ear Disorders
What are some pathology's of SSNHL? |
Viral - viral particles or Ab's have NOT been found in the cochlea
Bacterial Immune complexes Vascular (small vessel thrombosis, inner ear fibrosis, intravascular coagulopathy, or sludging) Trauma Barotrauma causing perilymph fistula Post-stapes surgery causing perilymph fistula Acoustic blast injury Temporal bone fxt Tumors: CPA, schwannomas, meningiomas, leptomeningeal carcinomatosis, metastatic dz Ototoxic meds Congenital inner ear deformities Intracochlear membrane rupture |
|
|
Inner Ear Disorders
Which lab tests should you consider in a pt with SSNHL? |
CBC with diff, sedimentation rate, coagulation studies, FTA, ABS-RPR, thyroid function, inner ear Ab, lipid profile
|
|
|
Inner Ear Disorders
What is the rate of spontaneous recovery in SSNHL? |
spontaneous recovery to 10 dB of opposite ear is 47-63%
|
|
|
Inner Ear Disorders
What are the S&Sx of perilymph fistula? |
sudden or progressive HL associated with roaring tinnitus, dysacusis, dysequilibrium
|
|
|
Inner Ear Disorders
What are the etiology's of perilymph fistulas? |
Stapes surgery
Trauma Exertion Barotrauma Spontaneous in chidlren or congenital HL |
|
|
Inner Ear Disorders
What is a positive Hennebert sign? |
It's a fistula tests = vertigo with pneumatic otoscopy
|
|
|
Inner Ear Disorders
What is the Tx for perilymph fistulas? |
Observation for 7-10 days; bed rest; head elevation; stool softner
Surgical indications = progressive HL with persistent sx |
|
|
Inner Ear Disorders
Describe sx of superior semicircular canal fistula What will the audiogram show? How do you repair this defect? |
vertical or vertical torsional nystagmus & vertigo induced by lifting, Valsalva or sound
Low-frequency CHL Tx - middle fossa repair of the fistula |
|
|
Inner Ear Disorders - Ototoxicity
What does the audiogram look like in aminoglycoside ototoxicity? |
High-freq progressing to all frequencies
|
|
|
Inner Ear Disorders - Ototoxicity
What does the audiogram look like in macrolide ototoxicity? |
bilateral flat SNHL
|
|
|
Inner Ear Disorders - Ototoxicity
What does the audiogram look like in salicylate ototoxicity? |
bilateral flat SNHL
|
|
|
Inner Ear Disorders - Ototoxicity
What does the audiogram look like in antineoplastic drug ototoxicity? |
high- and mid-frequency loss
|
|
|
Inner Ear Disorders - Ototoxicity
What does the audiogram look like in radiation ototoxicity? |
high- and mid-frequency loss, poor discrimination, progression to complete HL
|
|
|
Inner Ear Disorders
Where do the following tumors develop? Glomus tympanicum Glomus jugulare Glomus vagale |
Glomus tympanicum - on the promontory of the middle ear along the course of Arnold's nerve & Jacobson's nerve
Glomus jugulare - arising within the jugular bulb Glomus vagale - originates along vagus nerve |
|
|
Inner Ear Disorders
What are the S&Sx of glomus tumors? |
pulsating tinnitus
CHL (large tumors can cause SNHL) Cranial nerve palsy's (7, 9, 10, 11, 12) on exam - red, pulsating mass with "Brown" sign = blanching & pulsating seen with pneumatic otoscopy |
|
|
Posterior Fossa, CPA Tumors
What is the percentage of all intracranial tumors that are CPA tumors? |
10%
|
|
|
Posterior Fossa, CPA Tumors
What is the percentage of CPA tumors that are vestibular schwannoma's? How about meningioma's? |
Vestibular schwannoma's - 78%
Meningiomas - 3% |
|
|
Posterior Fossa, CPA Tumors
What are the S&Sx of CPA tumors? |
Unilateral progressive SNHL - 85%
Sudden HL - 15-20% (only 1-2% of pts with sudden HL have acoustic schwannoma) Tinnitus - 56% Vestibular dysfunction: vague disequilibrium - 50% Vertigo - 19% May also have midface hypesthesia, cranial nerve V dysfunction, facial paresis, diplopia, dysphagia, hoarseness, aspiration, cerebellar ataxia Hydrocephalus sx will include headache & vomiting |
|
|
Posterior Fossa, CPA Tumors
A pt with a CPA tumor has reduced sensation of the posterior external meatus. What is the name of this sign? |
Hitzelberger's sign - due to tumor pressuring against the facial nerve
|
|
|
Posterior Fossa, CPA Tumors
What kind of hearing loss can be expected in a pt with a CPA tumor? |
Usually high-frequency HL with reduced word recognition
|
|
|
Posterior Fossa, CPA Tumors
Name some audiometric signs that raise the index of suspicion of CPA tumors |
Asymmetric high-freq HL 15 dB
12% difference in word recognition Hearing complaints disproportional to audiologic findings Rollover - loss of word recognition with increased volume Acoustic reflex decay |
|
|
Posterior Fossa, CPA Tumors
Which imaging technique is able to detect internal auditory canal and CPA tumors less than 5 mm? |
MRI with and without gadolinium-DPTA contrast enhancement.
T2 fast spin echo MRI enhances fluid resolution, which contrasts contents of IAC...may be used to screen for acoustic schwannoma. |
|
|
Posterior Fossa, CPA Tumors
What does an acoustic schwanomma typically look like on imaging? How about meningioma? |
Acoustic schwannoma - will look like a "light bulb" centered at the IAC.
A meningioma will look like a broad based mass with a characteristic dural tail. Less involvement of IAC |
|
|
Posterior Fossa, CPA Tumors
What is the recommended observation time with MRI? |
Repeat MRI in 6 months and then annually with solid tumors
Repeat MRI every 4-6 months with tumors >1cm, cystic tumors or enlarging tumors |
|
|
Posterior Fossa, CPA Tumors
What is the usual rate of growth? |
Growth less than 0.2mm per year.
50-55% of small tumors (<1cm) show little or no growth in 1-3 yrs |
|
|
Posterior Fossa, CPA Tumors
What are the 3 different approaches you can take for surgical resection? |
Translabyrinthine apparch
Middle fossa approach Suboccipital, retrosigmoid approach |
|
|
Posterior Fossa, CPA Tumors
What are the indications for stereotactic radiosurgery for CPA tumors? |
Poor surgical candidates
Elderly Pt's who seek alternative to surgery Tumor size <2cm |