Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
What are three main types of severe rashes?
|
1. Auto immune
2. Severe coagulopathy related dermatoses 3. Vasculitis |
|
|
What are the mechanisms for skin blistering?
|
- Pressure: From friction, shearing force, blunt trauma
- Inflammation - Changes in tissue fluids (if blood, transudate enter) - Cell death (ex: TEN) - Deficient cellular attachment proteins (ex: autoimmune disease) |
|
|
What is direct vs. indirect immunofluorescence?
What pattern of IF is seen in bullous pemphigoid? What about pemphigus vulgaris? |
Direct= fluorescing antibody attaches to target
Indirect= primary antibody attaches to target, secondary fluorescing antibody attaches to primary Bullous--> linear, basement membrane Pemphigus --> mesh like pattern |
|
|
What do hemidesmosomes connect? What type of condition arises from antibodies to these proteins?
What special collagen is found that connects the DEJ? |
Hemidesmosomes- connect epidermal basement membrane to dermis.
Bullous pemphigoid= auto immune condition DEJ --> Type VII Collagen forms attachment |
|

What is this condition? What is the primary affected region?
|

Bullous pemphigoid Itense bullae on pink edematous plaque)
Antibodies to hemidesmosomes (BP AG1, BP AG2) |
|

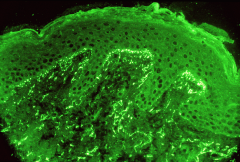
What is the most common autoimmune disease? How does it present on immunofluorescence stain using IgG and C3?
|
Bullous Pemphigoid
Direct IF shows linear pattern, staining basement membrane of epidermis |
|
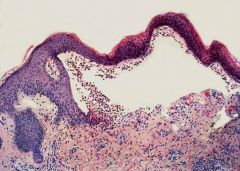
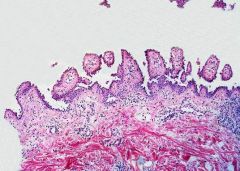
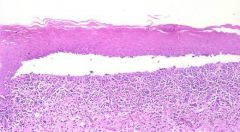
What is this a histologic picture of? How do you know?
|
Bullous pemphigoid
Affects the hemidesmosomes, so dermis is intact while the epidermis separates and interspace fills with fluid. Intraepithelial junctions intact. |
|
|
Describe the cascade of events that happens in bullous pemphigoid.
|
Autoantibody to BPAG1/2 binds
--> complement is activated --> Eos + Polys attracted --> protease released from leukocyte --> subepidermal blister formed |
|

What is Dermatitis Herpetiformis characterized by?
|
Antigen to TTGS (Tissue Transglutaminase 1). Patients have gluten hypersensitivity (celiac) and become ITCHY.
Small vesicles on knees, buttocks, face. However since people itch them, they present as 2nd lesion- crusts. |
|
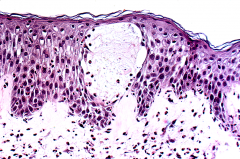
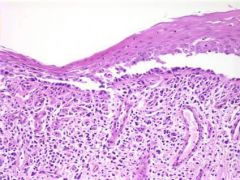
What is this a histologic picture of?
What would you expect the immunostain to look like? |
Dermatitis Herpetiformis (blistering in the dermal papilla).
Immunostain- shows granular IgA deposits in the dermal papilla. |
|
|
What is the principle defect in Epidermolysis bullosa?
If you see a person with ring shaped (annular) lesions that otherwise look like bullous pemphigoid, what condition might it be and what treatment would you employ? |
Epidermolysis Bullosa --> Collagen Type VII
Ring shapped bullae --> Linear IgA bullous dermatosis (treat with VANCOMYCIN!) |
|
|
What is the Nikolskly sign?
What about the Asboe-Hansen sign? |
Nikolsky: if you put pressure on normal skin near blister, will cause new blister
Asboe-Hansen: lateral pressure on intact blister causes it to spread. *both indicate INTRAEPIDERMAL blistering |
|
|
A positive Nikolsky sign indicates _______.
What is the principle target of autoimmunity in Pemphigus (in general)? |
+ Nikolsky = INTRAEPIDERMAL blistering (can also be positive in TEN where there is necrosis of epidermis)
Desmosomes (specifically Desmoglein) |
|
|
Name the antibody that is active in the following:
1. Pemphigus foliaceus 2. Pemphigus vulgaris (oral) 3. Pemphigus vulgaris (oral and skin lesion) |
1. Pemphigus foliaceous-- Desmoglein 1
2. Pemphigus vulgaris (oral)-- Desmoglein 3 3. Pemphigus vulgaris (oral, skin)--Desmoglein 3 and 1 |
|

What is this condition called? What specific antibodies are seen?
|
Pemphigus vulgaris (oral lesions only- so Desmoglein 3)
|
|
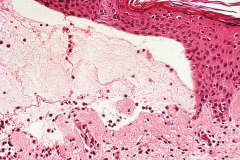
What is this a pathologic image of? What would the direct immunofluorescence stain look like?
|
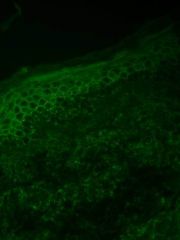
Pemphigus vulgaris (note that the basal layer is intact (hemidesmosomes intact) creating tombstone like single layer of cells.
The IF stain would show chicken wire/ mesh like appearance (because desmosomes envelop the keratinocytes) |
|

What type of bullae are seen in this condition? What is the Nikosky sign like?
|
Flaccid blisters, trunco-facial distribution. NON-INFLAMMATORY BULLAE. Erosions seen.
*always mucosal but not always skin involvement. + Nikolsky. |
|

What is this condition called? What specific antibody is generated in this condition?
|

Pemphigus foliaceus (looks like scaley, desquamating leaves).
Desmoglein 1 (NO ORAL LESIONS!) |
|
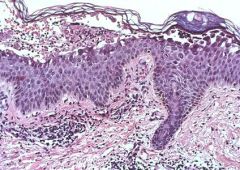
What is this a pathology picture of? What would it look like on direct immunofluorescence?
|

Pemphigus Foliaceous --> granular layer is blistering
DIF shows chicken-wire staining pattern that's SUPERFICIAL (in granular layer) |
|

A person comes in presenting with these oral hemorrhagic ulverating lesions that are refractory to treatment. Previously they were incorrectly diagnosed with Stevens-Johnson syndrome. They have not had any other problems to date.
What should you warn them about? |
PNP= Para neoplastic pemphigus = A blistering disease associated with intractable hemorrhagic mucositis (often oral).
*1/3rd PNP is presenting sign = i.e. warn them about possibility of a lymphoproliferative neoplasm |
|
What is characteristic about the pathology of Paraneoplastic Pemphigus (PNP)?
What antibodies are formed? |
Full range of pathology-->
- subepidermal blisters, intraepidermal blisters, and even lichenoid disease Remember, they have epitope escalation (so Desmoglein 1, 3, and plakin proteins and 170 kD antigen) |
|
|
What does PNP in children present as? What pulmonary condition can PNP present as?
|
PNP in children --> Castleman's
PNP in pulmonary --> BOOP (bronchiolitis obliterans with organizing pneumonia) |
|

What is this disease called? What gender is primarily affected? What might you note on physical exam?
|
Calciphylaxis (calcium deposition in media of dermal arteries)
F>M (3:1) Crunching upon palpation. |
|

What is this particular net-like pattern called and what does it signify?
|
Livedo reticularis- signifies arterial occlusion
NOT the same as calciphylaxis (there are many diseases, unfortunately, that can cause vascular occlusion) |
|
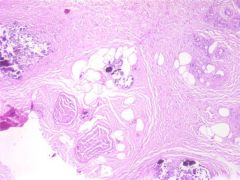
If you saw this biopsy what would you diagnose the patient with?
Given this condition, what other disease is the patient most likely suffering from? |
Calciphylaxis (this is calcium deposition)!
Person probably has chronic renal insufficiency (causing elevated PTH --> increase Ca2+ deposition in the wrong areas). |
|

A person comes in with this non-blanching red lesion. She has a fever. What should be your next steps as a medical student?
|

Purpura fulminans
- she has DIC and consumptive coagulopathy - inappropriately bleeding in body. Order blood cultures, broad spectrum Abx |
|
|
What is a primary and dangerous infectious cause of Purpura fulminans?
|
N. Meningitidis (meningococcus)
*Purpura: bleeding into skin, erythema, ecchymoses, purpuric plaque with thin border. |
|
|
What is the most common classification of Purpura fulminans?
What are other etiologies of purpura fulminans |
Most common= Acute infectious purpura fulminans (secondary sepsis and DIC).
Other etiologies: Protein C and S deficiencies, Idiopathic |
|

What is another name for Cutaneous Small Vessel Vasculitis (CSVV)?
What type of hypersensitivity reaction is it? Describe the pathogenesis |
Leukocytoclastic vasculitis (LCV)
Type III hypersensitivity --> Ag-Ab complex. When infection is present, increase vascular permeability allows Ag-Ab complexes to deposit between cells. Complement activated --> endothelial cell destruction and hemorrhage |
|
|
What is the etiology of CSVV?
|
MMSSHHCC
Meds, Malignancy Staph/Strep, Serum Sickness HCV/HBV, Henloch Schonlein purpura Cryoglobulinemia, CT tissue disease |
|

CSVV when systemic manifests in what systems? What workup would you do for someone with CSVV?
|
Kidney, GI, Nervous
- UA - Stool guiac - Follow for CNS abnormalities |