Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
158 Cards in this Set
- Front
- Back
|
Clinical Attachment Level
|
the probing depth measured from a fixed point, such as the cementoenamel junction; CAL
|
|
|
Diastema
|
a space between two natural adjacent teeth
|
|
|
Hyperkeratosis
|
abnormal thickening of the keratin layer (stratum corneum) of the epithelium
|
|
|
Hyperplasia
|
abnormal increase in volume of a tissue organ caused by formation and growth of new normal cells
|
|
|
Hypertrophy
|
increase in size of tissue or organ caused by an increase in size of its constituent cells
|
|
|
Keratinization
|
development of a horny layer of flatttened epithelial cells containing keratin
|
|
|
Mastication
|
act of chewing
|
|
|
Pus
|
a fluid product of inflammation that contains leukocytes, degerated tissue elements, tissue fluids, and microorganisms
|
|
|
Stippling
|
the pitted, orange-peel appearance frequentlyseen on the surface of the attached gingiva
|
|
|
Suppuration
|
formation of puss
|
|
|
Clinical crown
|
the part of the crown of a tooth that can be seen by the clinician
|
|
|
Clinical root
|
the part of the root of a tooth that can bee seen by the clinician
|
|
|
Anatomical crown
|
the part of the tooth covered in enamel
|
|
|
Anatomical root
|
the part of the tooth coverd in cementum
|
|
|
Masticatory Mucosa
|
covers gingiva and hard palate and is firmly attached; keratinized
|
|
|
Lining mucosa
|
covers inner surfaces of the lips and cheeks, floor of mouth, under side of tongue, soft palate, and alveolar mucosa; not keratinized
|
|
|
Specialized mucosa
|
covers dorsum (upper surface) of tongue; composed of papillae
|
|
|
Types of specialized mucosa
|
filiform, fungiform, circumvallate, foliate
|
|
|
Filiform papillae
|
most numerous, no taste buds
|
|
|
Fungiform
|
mushroom shaped, more red and contains taste buds
|
|
|
Circumvallate papillae
|
10-14 large round papillae in a V shape
contains taste buds |
|
|
Foliate papillae
|
on lateral posterior sides of tongue; no taste buds
|
|
|
What kind of tissue are periodontal ligaments made up of?
|
fibrous connective tissue
|
|
|
What do periodontal ligaments do?
|
surround and connecta the alveolar bone to the roots of the teeth
|
|
|
Where are periodontal ligaments located?
|
in the periodontal space between the cementum and alveolar bone
|
|
|
Sharpey's fibers
|
fibers that are inserted into the cemetum on one side and alveolar bone on the other
|
|
|
What are the five GINGIVAL fiber groups of the periodontium?
|
Dentogingival, alveologingival, cercumferential, dentoperiosteal, transseptal
|
|
|
What are the four PRINCIPAL fiber groups?
|
apical, oblique, horizontal, alveolar crest
|
|
|
Dentogingival fibers
|
cementum to free gingiva
|
|
|
Alveologingival fibers
|
alveolar crest to free and attached gingiva
|
|
|
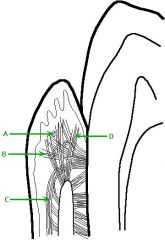
A: Circumferential fibers
B: Dentogingival fibers C: Alveologingival fibers D: Dentoperiosteal fibers |
|
|
Circumferential fibers
|
around the neck of the tooth
|
|
|
Dentoperiosteal fibers
|
cervical cementum over the alveolar crest
|
|
|
Transseptal fibers
|
cervical area of one tooth across to an adjacent tooth
|
|
|
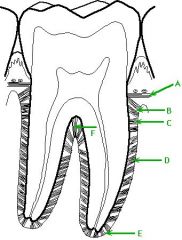
Apical fibers
|
root apex to surrounding bone
|
|
|
Oblique fibers
|
root above apical fibers obliquely toward the occlusal
|
|
|
Horizontal fibers
|
cementum in the middle of each root to adjacent alveolar bone
|
|
|
Alveolar crest fibers
|
alveolar crest to cementum just below CEJ
|
|
|
A: Transseptal fibers
B: Alveolar crest fibers C: Horizontal fibers D: Oblique fibers E: Apical fibers F:Interradicular fibers |
|
|
Cementum
|
layer of calcified connective tissue that covers the root of the tooth
|
|
|
Function of cementum (2)
|
to seal tubules of dentin and to provide attachment for fibers; not sensitive
|
|
|
How thick is cementum?
|
about 50 to 200 micrometers about the apex and 30-60 about the cervical are
|
|
|
Alveolar bone
|
consists of lamina dura which surrounds the tooth socket and supporting bone
|
|
|
Gingiva
|
surrounds the necks of teeth and is attached to the teeth and alveolar bone
|
|
|
What three parts is the gingiva made up of?
|
free gingiva, attached gingiva, and interdental gingiva
|
|
|
Free gingival groove
|
a shallow linear groove that demarcates the free from the attached gingiva
|
|
|
Gingival sulcus
|
the crevice or groove between the free gingiva and the tooth
|
|
|
Inner boundary of gingival sulcus
|
tooth surface; could be enamel, cementum, or both
|
|
|
Outer boundary of gingival sulcus
|
Sulcular epithelium
|
|
|
Base of gingival sulcus
|
coronal margin of tha ttached tissues; also called the probing depth or bottom of the pocket
|
|
|
Healthy sulcus depth minimum
|
0.5 mm
|
|
|
Average depth of healthy sulcus
|
1.8 mm
|
|
|
Healthy readings for depth of healthy sulcus
|
1-3 mm
|
|
|
Junctional epithelium
|
cufflike band of stratified squamous epithelium that is continuous witht he sulcular epithelium and completely encircles the tooth; not keratinized
|
|
|
Size of Junctional epithelium
|
up to 15-20 cells at sulcular epithelium down to 1-2 cells at apical end
|
|
|
Interdental papillae
|
gingival occupying the interproximal area between two adjacent teeth; also called embrasure
|
|
|
Type 1 embrasure
|
gingival tissue fills area; pyramidal
|
|
|
Type 2 embrasure
|
slight to moderate recession; blunted
|
|
|
Type 3 embrasure
|
extensive recession or complete loss; absent
|
|
|
Col
|
depression between the lignal or palatal and facial papillae that conforms to the proximal contact area
|
|
|
Where do most periodontal infections start?
|
Col area
|
|
|
Attached gingiva
|
continuous with the oral epthelium of the free gingiva and is covered with keratinized stratified squamous epithelium cells
|
|
|
How is attached gingiva attached?
|
firmly bound to the underlying cementum and alveolar bone
|
|
|
Mucogingival junction
|
a line that marks the connection between the attached gingiva and the alveolar mucosa
|
|
|
Alveolar mucosa
|
movable tissue with smooth, shiny surface; nonkeratinized
|
|
|
Clinically normal gingival tissue
|
pale or coral pink pigment, knife edged, stippling, firm, no bleeding
|
|
|
Gingival examination
|
examine color, shape, consistency, surface texture, position, bleeding, exudates
|
|
|
Healthy gingiva in children
|
pink, thick, rounded or rolled, not tightly adapted to teeth, may not have stippling,
|
|
|
Explorer
|
a slender stainless steel instrument with a fine flexible sharp point used for examination of the surfaces of the teeth to detect irregularities
|
|
|
Fremitus
|
a vibration perceptible by palpation
|
|
|
Probe
|
smooth, slender instrument usually round in diameter with a rounded tip designed for examination of the teeth and soft tissues; except for a few probes made only for blunt examination, probes are calibrated in millimeter increments to facilitate recordings for comparisn with periodic assessment
|
|
|
Probing depth
|
the distance from the gingival margin to the location of the periodontal probe tip at the coronal border of attached periodontal tissues
|
|
|
Mirror surfaces (3)
|
Plane, concave, front surface
|
|
|
Plane mirror surface
|
may produce double image
|
|
|
Concave mirror surface
|
magnifying
|
|
|
Front surface mirror surface
|
reflecting surface is on the front of the lense rather than on the back
|
|
|
Purposes of the mouth mirror (4)
|
indirect vision, indrect illumination, transillumination, retraction
|
|
|
Uses of air water syringe
|
Improve and facilitate procedures, improve visibility of treatment area, prepare teeth for certain procedures
|
|
|
Probe characteristics
|
straight working end
|
|
|
Pocket
|
diseased gingival sulcus
|
|
|
How is a pocket measured?
|
from base of pocket to gingival margin
|
|
|
How are proximal surfaces approached?
|
by entering from both the facial and lingual aspects of a tooth
|
|
|
Where is the probe stopped in normal healthy tissue?
|
base of sulcus at the coronal end of junctional epithelium
|
|
|
Where is the probe stopped in gingivitis and early periodontitis?
|
within junctional epithelium
|
|
|
Where is the probe stopped in advanced periodontitis?
|
probe tip passes through junctional epithelium and reaches attached connective tissue fibers
|
|
|
How do you line the probe up to get an accurate reading?
|
with the long axis of the tooth
|
|
|
Purposes and uses of an explorer (5)
|
detect texture of tooth surfaces, subgingival tooth surfaces, define extent of instrumentation needed, evaluate treatment
|
|
|
Tooth surface irregularities
|
deposites, anomalies (enamel pearls), restorations, demineralization, restoration
|
|
|
Angular or vertical bone loss
|
reduction in height of crestal bone that is irregular; commonly localized
|
|
|
Furcation involvement
|
when a pocket extends into a furcation area
|
|
|
Periodontal ligament space
|
connective tissue that appears radiolucent on a radiograph
|
|
|
Edema
|
accumulation of excessive fluid in cells, tissues, or a serous cavity
|
|
|
Gingivitis
|
inflammation of the gingival tissues
|
|
|
Iatrogenic
|
resulting from treatment by a professioal person
|
|
|
Lesion
|
any pathologic or traumatic discontinuity of tissue or loss of function of a part; broad term including wounds, sores, ulcers, tumors, and any other tissue damage
|
|
|
Periodontitis
|
inflammation in the periodontium affecting gingival tissue, periodontal ligament, cementum, and supporting bone
|
|
|
Permeable
|
permitting passage of fluid
|
|
|
Refractory
|
not readily responsive to treatment
|
|
|
Toxin
|
a poison; protein produced by certain animals, higher plants, and pathogenic bacteria
|
|
|
Xerostomia
|
dryness of the mouth from a lack of normal secretions
|
|
|
Initial lesion
|
occurs within 2 to 4 days of irritation, fluid fills the spaced in the connective tissue
|
|
|
Early lesion
|
Biofilm becomes older and thicker within 7 to 14 days, breakdown to the support at gingival margin
|
|
|
Established lesion
|
Fluid migration into tissues and sulcus increase; plasma cells = area of chronic inflammation; pocket epithelium is more permeable, early pocket formation
|
|
|
Advanced lesion
|
bacteria enter sulcus and provide subgingical boifilm; inflammation spreads resulting in bone loss
|
|
|
Gingival pocket
|
pocket formed by gingival enlargement without apocal migration of the junctional epithelium
|
|
|
Periodontal pocket
|
result of disease or degeneration that caused the junctional epithelium to migrate apically along the cementum
|
|
|
Suprabony
|
base of pocket is coronal to the crestof the alveolar bone
|
|
|
Intrabony
|
base of pocket is below or apical to the crest of alveolar bone
|
|
|
What substances are found in a pocket?
|
subgingival biofilm, microorganisms, gingival sulcus fluid, desquamated epithelial cells, leukocytes, purulent exudate
|
|
|
Small amount of dentin exposed in __% of teeth
|
10%
|
|
|
Cementum and enamel meet in __% of teeth
|
30%
|
|
|
Cementum overlaps enamel in __% of teeth
|
60%
|
|
|
Complications of pocket formation
|
furcation involvement and mucogingival involvement
|
|
|
Class I furcation involvement
|
early beginning involvement; probe can enter furcation area and feel anatomy of roots
|
|
|
Class II furcation involvement
|
Moderate involvement; probe can enter but cannot pass through
|
|
|
Class III furcation involvement
|
Severe involvement; probe can be passes between roots through the entire furcation
|
|
|
Class IV furcation involvement
|
exposure of furcation; probe can pass through entire furcation
|
|
|
Mucogingival involvement
|
a pocket that extends to or beyond the mucogingival junction and into the alveolar mucosa
|
|
|
Functions of attached gingiva
|
supports, withstands stress, provides attachment
|
|
|
Factors involved in disease development (4)
|
Etiologic, predisposing, contributing, risk
|
|
|
Etiologic factor
|
factor that is the actual cause of a disease or condition
|
|
|
Predisposing factor
|
factor that redners a person susceptible to a disease or condition
|
|
|
Contribution factor
|
factor that lends assistance to, supplements, or adds to a condition or disease
|
|
|
Risk factor
|
an exposure that increases the probability that disease will occur
|
|
|
Dental factors (4)
|
tooth surface irregularities, tooth contour, tooth position, dental prostheses
|
|
|
Gingival factors (3)
|
position, size and contour, and effect of mouth breathing
|
|
|
Other factors that contribute to disease development (2)
|
personal oral care and diet and eating habits
|
|
|
Self cleansing mechanisms (3)
|
saliva, tongue, morphology of teeth
|
|
|
Risk factors for periodontal disease (5)
|
Drugs, tobacco, diabetes, osteoporosis, and psychosocial factors
|
|
|
Amelogenesis
|
production and development of enamel
|
|
|
Dental caries
|
disease of the mineralized structures of the teeth characterized bu demineralization of the hard components and dissolution of the organic matrix
|
|
|
Arrested caries
|
carious lesion that has become stationary and does not show a tendency to progress further; frequently has a hard surface and takes on a dark brown or reddish-brown color
|
|
|
Primary caries
|
occurs on a surfae not previously affected; also called initial caries; early lesion may be referred to as incipient caries
|
|
|
Rampant caries
|
widespread formation of chalky white areas and incipient lesions that may increase in size over a comparatively short time
|
|
|
Recurrent caries
|
occurs on a surface adjacent to a restoration; may be a continuation of the original lesion; also called secondary caries
|
|
|
endentulous
|
without teeth
|
|
|
Exfoliation
|
lossof primary teeth following physiologic resorption of root structures
|
|
|
Idiopathic
|
denoting a condition of unknown cause
|
|
|
Incipient
|
beginning; coming into existence
|
|
|
Resorption
|
removal of bone or tooth structure; gradual dissolution of the mineralized tissue; may be internal or external; occurs during exfoliation of a primary tooth and from the pressure of orthodontic treatment
|
|
|
Requirements for Dental caries (3)
|
microorganisms, carbohydrate, and susceptible tooth surface
|
|
|
Acid forming bacteria in dental biofilm
|
mutans streptococci and lactobacilli
|
|
|
Simple cavity
|
one tooth surface
|
|
|
compound cavity
|
two tooth surfaces
|
|
|
complex
|
more than two tooth surfaces
|
|
|
Phase I: incipient lesion; Enamel caries (4)
|
subsurface demineralization, visualization, first clinical evidence, reminerilization
|
|
|
Phase II: untreated incipient lesion; Enamel caries (3)
|
Breakdown of enamel, progression of carious lesion, spread of carious lesion
|
|
|
Pit and fissure dental caries
|
begins in a minute fault in the enamel where 3 or more lobes of tooth meet irregularly
|
|
|
Smooth surface dental caries
|
begin in smooth surfaces where there is no pit, groove, or other fault; occurs where biofilm is protected from removal
|
|
|
Early childhood caries
|
caused by baby bottle syndrome
|
|
|
Root caries
|
increases with age but not because of age, lesion of cementum and dentin
|
|
|
Types of noncarious dental lesions (6)
|
enamel hypoplasia, attrition, erosion, abrasion, fractures, abfraction
|
|
|
Enamel hypoplasia
|
defect that occurs as a result of a disturbance in the formation of the organic enamel matrix
|
|
|
Attrition
|
wearing away of a tooth as a result of tooth to tooth contact
|
|
|
Erosion
|
loss of tooth substance by a chemical process that does not involve known bacterial action
|
|
|
Abrasion
|
mechanical wearing away of tooth substance by forces other than mastication
|
|
|
Fractures
|
caused by trauma to the face
|
|
|
Abfraction
|
a wedge shaped lesion with sharp line angles at the cervical region of the dentition. caused bu stresses resulting from biomechanical loading forces on the teeth.
|