Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
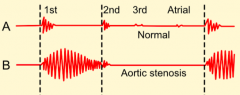
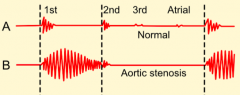
What are the systolic murmurs?
|
- Aortic Stenosis
- Mitral Regurgitation |
|
|
What are the diastolic murmurs?
|
- Aortic Regurgitation
- Mitral Stenosis |
|
|
What does Aortic Regurgitation hate?
|
Bradycardia
|
|
|
What does Mitral Stenosis hate?
|
Tachycardia
|
|
|
Which of the murmurs hate a slow HR or a fast HR?
|
- Aortic Regurgitation hates Bradycardia
- Mitral Stenosis hates Tachycardia |
|
|
What is the most common cause of aortic stenosis?
|
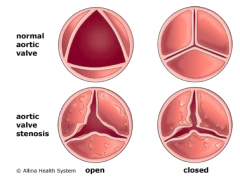
Calcific Degeneration:
- <65 yo: usually to bicuspid valve (if <30, almost always) - >65 yo: probably tricuspid valve |
|
|
What is notable about the pressure vs time curve for a normally functioning aortic valve?
|

All the pressure from the ventricle gets transferred to the aorta (no resistance to blood flow by aortic valve)
|
|
|
What is notable about the pressure vs time curve for an aortic valve with stenosis?
|
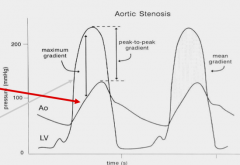
- Pressure in ventricle highly exceeds pressure in aorta
- This means that the aortic valve is limiting the transfer of pressure from LV to aorta |
|
|
Does aortic stenosis cause a pressure or volume overload state? What does this cause?
|
Pressure overload → Hypertrophy (sarcomeres in parallel)
|
|
|
What does the Pressure-Volume loop for an aortic valve with stenosis tell you?
|
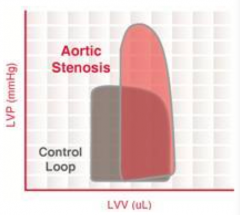
- Ventricle is squeezing, but volume is staying the same valve is stenosed
- Causes increase in pressure above normal - Eventually pressure in ventricle exceeds pressure in aorta and some blood gets out - There is a smaller stroke volume |
|
|
What physical exam features will you notice for aortic stenosis?
|
- Sustained LV impulse
- No / little LV displacement - Pulsus Parvus et Tardus (slow and delayed upstroke of carotid impulses) - Absent A2 or paradoxically split A2 - Murmur is systolic crescendo decrescendo (later peaking is associated with worse stenosis) |
|
|
What valve pathology is associated with Pulsus Parvus et Tardus? What does this mean?
|
- Aortic Stenosis
- Slow and delayed upstroke of carotid impulses |
|
|
What valve pathology is associated with a systolic crescendo-decrescendo murmur?
|
Aortic Stenosis - late peaking indicates worse stenosis
|
|
|
Describe the typical murmur for Aortic Stenosis.
|
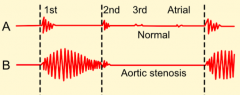
- Absent A2 or paradoxically split A2
- Systolic murmur with crescendo decrescendo |
|
|
Describe the typical chest x-ray for Aortic Stenosis.
|
- Little cardiac enlargement due to LVH
- Post-stenotic dilation of the ascending aorta - Ca2+ on aortic valve |
|
|
What is the mean survival for patients with the following symptoms from their Aortic Stenosis?
- Angina? - Syncope? - CHF? |
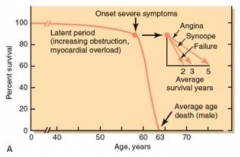
- Angina: 5 years
- Syncope: 3 years - CHF: 2 years |
|
|
Should a patient without symptoms from their aortic stenosis be worried about dying?
|
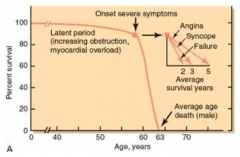
No, you don't have a shortened lifespan until you start getting symptoms:
- Angina: 5 years - Syncope: 3 years - CHF: 2 years |
|
|
What is the size of the valve opening for the different severities of aortic stenosis?
|
- Mild: >1.5 cm2
- Moderate: 1-1.5 cm2 - SEVERE: <1 cm2 |
|
|
When should you get an aortic valve replacement for Aortic Stenosis?
|
** Symptomatic patients w/ severe AS (valve opening <1 cm2)
- Patients w/ severe AS undergoing CABG - Patients w/ severe AS undergoing surgery on aorta or other heart valves - Patients w/ severe AS and LV systolic dysfunction (ejection fraction < 50%) |
|
|
What life-prolonging treatment(s) are there for Aortic Stenosis?
|
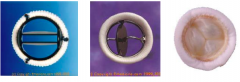
Only valve replacement
|
|
|
Does mitral regurgitation cause a pressure or volume overload state? What does this cause?
|
Volume overload
- Tolerated well until severe - When severe regurgitation develops slowly enough, patients can often tolerate well for extended periods |
|
|
What is the most damaging to organ systems: rate of change or degree of change?
|
Rate of change is the most important factor for organ damage
|
|
|
What is notable about the pressure vs time curve for a mitral valve with regurgitation
|
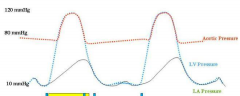
- Pressure transfer from LV to Aorta is normal
- The LA pressure increases more than it should d/t blood returning from LV → LA |
|
|
What does the Pressure-Volume loop for a mitral valve with regurgitation tell you?
|
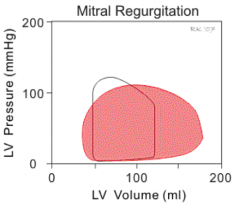
- There is no point in time when both mitral and aortic valves are completely shut
- Therefore, there are no iso-volumic parts of curve - LV volume gets higher because more blood is staying in heart (original blood to get pumped into LV + blood that regurgitated back and is getting pumped back in) - Leads to greater contraction (Frank-Starling mechanism) because it is stretched out more → increased SV |
|
|
Describe the typical murmur for Mitral Regurgitation.
|
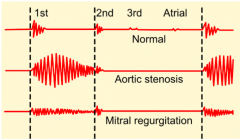
Throughout all of systole you have fluid going from LV to LA at constant rate = Holosystolic Murmur
|
|
|
What symptoms are noted with chronic Mitral Regurgitation?
|
- Exertional symptoms are most common
- Heart can change without symptoms (well-tolerated until severe) |
|
|
What are some causes of primary (organic) mitral valve pathology?
|
- Myxomatous disease - degenerative
- Rheumatic valve disease - Endocarditis - Congenital (cleft leaflet) |
|
|
What are some causes of secondary (functional) mitral valve pathology?
|
- Ischemic Cardiomyopathy
- Dilated Cardiomyopathy - Hypertrophic Cardiomyopathy |
|
|
How should you manage mitral regurgitation?
|
Management based on:
- Development of symptoms - Loss of LV systolic function |
|
|
What is the most common cause of Mitral Stenosis?
|
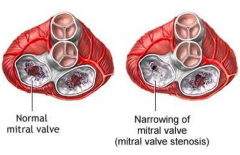
Rheumatic Fever / immune disease
|
|
|
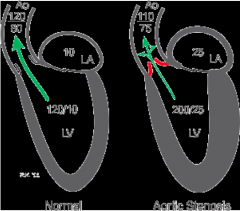
What happens to the pressures when there is Mitral Stenosis?
|
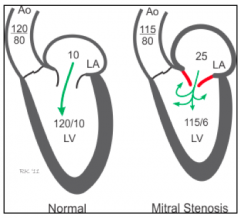
- Pressure increases in LA to push blood into LV
- This can increase the pressure in the lungs → pulmonary edema |
|
|
What is the normal size opening to the Mitral Valve? What is the size with mitral stenosis?
|
- Normal: 3-4 cm2
- MS: < 2 cm2 - Severe MS: < 1 cm2 |
|
|
When do you get symptoms of pulmonary congestion with Mitral Stenosis?
|
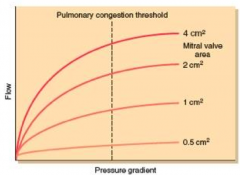
- At smaller valve size openings, the pressure increases to try to maintain flow across mitral valve
- Once you exceed a certain level of pressure (for any valve size) you will get pulmonary congestion - It is easy to exceed this threshold when the valve size is severely limited (possibly even at rest) |
|
|
What are the symptoms of Mitral Stenosis?
|
- Predominantly exertional
- Atrial fibrillation evolves - Severe pulmonary hypertension w/ RH failure eventually (because RH has to push really hard to get blood to go into LH which has increased pressure) |
|
|
Describe the typical murmur for Mitral Stenosis.
|
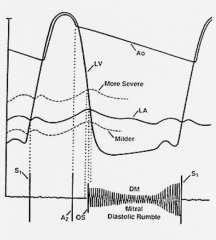
- Early: opening snap and diastolic murmur
- Late: opening snap and diastolic murmur w/ RV lift - Snap is high pitched - Murmur is low pitched = diastolic rumble |
|
|
How do you confirm the diagnosis of Mitral Stenosis?
|
- Echo Lab
- Cardiac Catheterization Lab Severe MS: - MVA (mitral valve area) ≤ 1 cm2 - MVG (mean valve gradient) ≥ 10 mmHg |
|
|
What do you seen on EKG of Mitral Stenosis?
|
Hockey stick shape in mitral valve
|
|
|
How do you treat Mitral Stenosis?
|
- Balloon Valvuloplasty
- Valve Replacement |
|
|
What can cause Aortic Regurgitation?
|
- Endocarditis
- Trauma - Dissection of aorta |
|
|
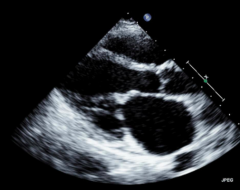
What happens to the heart with chronic aortic regurgitation?
|
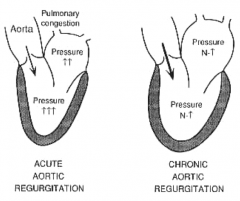
Heart gets REALLY BIG (largest dilation of heart) = "Cor Bovinum"
|
|
|
What valve pathology is associated with "Cor Bovinum" = cow heart?
|

Aortic Regurgitation
|
|
|
What does the Pressure-Volume loop for an aortic valve with regurgitation tell you?
|
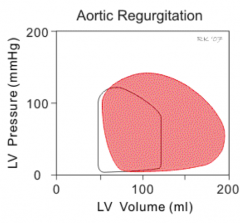
- No isovolumic phase because there is never a time when both valves are closed
- Increased LV pressure (compared to mitral regurgitation) |
|
|
What are the symptoms / tolerance of Aortic Regurgitation?
|
- When progression to severe is slow, chronic severe aortic regurgitation is very well tolerated
- When symptoms evolve, they are usually exertional - Sometimes there is loss of systolic function while patient remains asymptomatic |
|
|
What will you notice on physical examination of Aortic Regurgitation?
|
- Widened pulse pressures
- Diffuse and displaced Point of Maximal Impulse (PMI) - Diastolic murmur (diastolic decrescendo murmur as they lean forward and exhale) - De Musset's sign: head bobbing - Muller's sign: bobbing uvula - Quinicke's sign: blanching nail beds |
|
|
What are the peripheral signs of aortic regurgitation?
|
- De Musset's sign: head bobbing
- Muller's sign: bobbing uvula - Quinicke's sign: blanching nail beds |
|
|
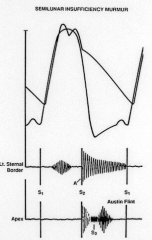
Describe the typical murmur for Aortic Regurgitation.
|
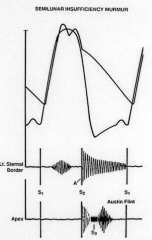
Diastolic Decrescendo murmur best heard as they lean forward and exhale
|
|
|
What are they signs indicative of?
- De Musset's sign: head bobbing - Muller's sign: bobbing uvula - Quinicke's sign: blanching nail beds |
Aortic Regurgitation
|
|
|
How do you treat Aortic Regurgitation?
|
Valve replacement
|