Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
131 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What are the criteria for a febrile seizure?
|
1. age 3 m/o to 6 y/o (most common between 6-18 months)
2. fever > 38.8°C 3. non-CNS infection |
|
|
|
Define aphasia.
|
variety of language disorders
inability to speak, write, or comprehend language d/t brain disorder |
|
|
|
What are the most common causes of febrile seizures?
|
usually acute respiratory illness
sometimes gastroenteritis (Shigella, Campylobacter), UTI rarely roseola infantum, immunizations |
|
|
|
Define hypersomnia.
|
excessive daytime sleepiness
|
|
|
|
FEBRILE SEIZURES:
|
ETIOLOGY:
Criteria: 1. age 3 m/o to 6 y/o (most common between 6-18 months) 2. fever > 38.8°C 3. non-CNS infection Causes: usually d/t acute respiratory illnesses sometimes d/t gastroenteritis (Shigella, Campylobacter), UTI rarely d/t Roseola infantum (classic cause), immunizations occur in 2-3% of children CLINICAL PRESENTATION: 90% generalized, last <5 min, occur early in illness causing fever DIAGNOSTIC WORKUP: evaluate for source of fever and R/O CNS infection (meningitis, encephalitis) CBCDP and BC LP → if child < 18 months (since signs unreliable), cause of fever not found, close F/U not possible, or recovery slow (negative finding does not R/O emerging CNS infection) MANAGEMENT: 1. find source of fever and treat appropriately 2. measures to control fever (tepid baths, antipyretics, antibiotics) are reasonable but unproven to prevent recurrent febrile seizures 3. if complicated seizure or medical reassurance fails to relieve family anxiety → anticonvulsant prophylaxis (phenobarbital, valproic acid) PATIENT EDUCATION: 1. recurrent febrile seizures occur in 30-50% of cases → expect more seizures 2. simple febrile seizures do not have any long-term adverse outcomes 3. complex febrile seizures may rarely lead to epilepsy (occur in 1-3%; risk increased 2-5 times; risk higher if complex features such as longer than 15 minutes, more than 1 seizure daily, focal features; risk higher if abnormal neurologic status preceding seizure, onset before age 1, FH of epilepsy) |
|
|
|
Define hemiplegia.
|
paralysis of one side of body
|
|
|
|
Define paraplegia.
|
paralysis of lower half of body
d/t thoracic spinal cord injury |
|
|
|
Define quadriplegia.
|
partial or total paralysis of entire body from neck down
d/t cervical spinal cord injury |
|
|
|
Define decorticate.
|
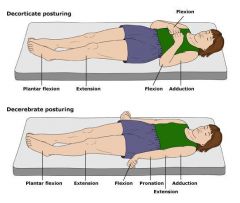
abnormal posturing characterized by:
rigidity adduction of arms flexion of elbows clenched fists extension of legs plantar flexion |
|
|
|
Define decerebrate.
|
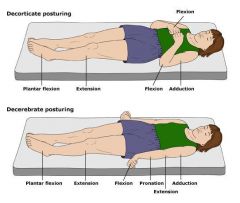
abnormal posturing characterized by:
rigidity head/neck arched back arms adducted elbows extended and pronatated clenched fists legs extended plantar flexion |
|
|
|
CLUSTER HEADACHE:
|
ETIOLOGY:
unknown PREVALENCE: Middle-aged men CLINICAL PRESENTATION: episodes of severe unilateral periorbital pain occurring daily x several weeks often accompanied by ipsilateral nasal congestion, rhinorrhea, lacrimation, eye redness, and Horner syndrome restlessness, agitation during attacks episodes often occur at night, awaken patient, last 15 min to 3 hours, followed by spontaneous remission that may last weeks to months triggers include alcohol, stress, glare, specific foods no signs apart from Horner syndrome DIAGNOSTIC WORKUP: none MANAGEMENT: PATIENT EDUCATION: |
|
|
|
List the different types of seizures.
|
generalized seizures:
absence (petit mal) tonic-clinic (grand mal) partial seizures: simple partial complex partial |
|
|
|
What is the difference between a simple partial and complex partial seizure
|
both affect restricted part of one cerebral hemisphere
both may become secondarily generalized leading to a tonic, clonic, or tonic-clonic seizure consciousness preserved in simple partial consciousness impaired in complex partial |
|
|
|
What is the difference between a partial seizure and a generalized seizure?
|
partial seizures involve localized are of the brain and only 1 cerebral hemisphere; consciousness may be preserved or impaired
generalized seizures involve diffuse area of the brain and both cerebral hemispheres; consciousness may be impaired or lost |
|
|
|
Define seizure.
|
abnormal paroxysmal neuronal discharge in the brain causing transient disturbance in cerebral function
|
|
|
|
Define epilespy.
|
recurrent unprovoked seizures
|
|
|
|
What is a complex seizure?
|
restricted part of one cerebral hemisphere affected
may become secondarily generalized leading to a tonic, clonic, or tonic-clonic seizure consciousness impaired (may be preceded by illusions, hallucinations, automatisms) |
|
|
|
What is a partial seizure?
|
restricted part of one cerebral hemisphere affected
may become secondarily generalized leading to a tonic, clonic, or tonic-clonic seizure consciousness preserved may manifest as focal motor symtoms (convulsive jerking), somatosensory symptoms (paresthesias), special sensory symptoms (light flashes, buzzing), autonomic symptoms (abnormal epigastric sensations, sweating, flushing, pupillary dilation), dysphasia, déjà vu , illusions or hallucinations |
|
|
|
What are the causes of seizures?
|
idiopathic → usually occurs between 5-20y/o
congenital abnormalities perinatal injuries trauma vascular → usually occur >60y/o metabolic disorders → hypo/hyperglycemia, uremia infectious disease → meningitis, encephalitis, neurosyphilis neoplasm → usually occur >30y/o degenerative drug withdrawal |
|
|
|
LACUNAR INFARCT:
|
small lesions (usually < 5 mm in diameter)
occur in the distribution of short penetrating arterioles in the basal ganglia, pons, cerebellum, anterior limb of the internal capsule, and, less commonly, the deep cerebral white matter associated with poorly controlled HTN or DM, associated with several clinical syndromes → contralateral pure motor or pure sensory deficit, ipsilateral ataxia with crural paresis, and dysarthria with clumsiness of the hand neurologic deficit may progress over 24–36 hours before stabilizing sometimes visible on CT scans → small, punched-out, hypodense areas prognosis good, often with partial or complete recovery within 4-6 weeks |
|
|
|
Which is more sensitive for detecting acute blood, CT or MRI?
|
CT
|
|
|
|
Which should be ordered for suspected hemorrhagic stroke?
|
CT
|
|
|
|
What is a subarachnoid hemorrhage?
|
leakage of blood into subarachnoid space
|
|
|
|
What is the diagnostic workup of subarachnoid hemorrhage?
|
non-contrast CT
LP if CT negative but still highly suspicious |
|
|
|
Worst HA of your life describes?
|
subarachnoid hemorrhage?
|
|
|
|
What is the most common cause of subarachnoid hemorrhage?
|
70% caused by aneurysm
|
|
|
|
Subarachnoid hemmorhage is indicated by what LP results?
|
presence of RBCs and xanthochromia
|
|
|
|
What are the risk factors of subarachnoid hemorrhage?
|
smoking
HTN FH |
|
|
|
Where do saccular aneurysms tend to occur?
|
arterial bifurcations
usually anterior Circle of Willis specifically anterior or posterior communicating arteries, bifurcation of the middle cerebral artery, or bifurcation of the internal carotid artery |
|
|
|
INTRACRANIAL ANEURYSM:
|
ETIOLOGY:
may be associated with polycystic kidney disease, coarctation of the aorta RISK FACTORS: smoking, HTN, hypercholesterolemia increased risk of subarchnoid hemorrhage associated with older age, female, non-white, HTN, hypercholesterolemia, high alcohol consumption (>150g/week), tobacco smoking, previous sxs, posterior circulation aneurysms, larger aneurysms CLINICAL PRESENTATION: usually asymptomatic possible focal neurologic deficit d/t compression on adjacent structures DIAGNOSTIC WORKUP: angiography → bilateral carotid and vertebral studies INITIAL MANAGEMENT: prevent hemorrhages prompt tx if symptomatic or large → surgery or endovascular observation with arteriography if asymptomatic and small (<10mm) PREVENTION: PROGNOSIS: may rupture producing subarachnoid hemorrhage |
|
|
|
What are AV malformations?
|
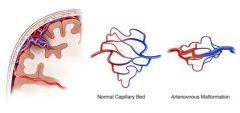
congenital vascular malformations consisting of abnormal arteriovenous communications without intervening capillaries
|
|
|
|
What is the etiology of Tourette's syndrome?
|
autosomal dominant genetic disorder
|
|
|
|
What is the Rx management of Tourette's syndrome?
|
haloperidol
|
|
|
|
What is oculogyric crisis?
|
type of ocular dystonic reaction
|
|
|
|
What are the characteristics of an oculogyric crisis?
|

onset may be paroxysmal or stuttering over several hours
initial symptoms include malaise, restlessness, agitation, or fixed stared usually SUSTAINED MAXIMAL UPWARD DEVIATION OF EYES BILATERALLY occasionally eyes may deviated upward and laterally, deviated downward, or converge protracted staring episodes periorbital twitches blepharospasm ocular pain widely opened mouth tongue protrusion extension or lateral flexion of neck wave of exhaustion following episode eye blinking, lacrimation, pupil dilation, drooling, facial flushing, vertigo |
|
|
|
What is ddx for oculogyric crisis?
|
usually d/t neuroleptic drugs
other drugs (benzodiazepines, lithium, carbamazepine, levodopa, metoclopramide, nifedipine, cetirizine, amantadine, chloroquine) head trauma meningitis encephalitis focal seizures conversion reaction other movement disorders |
|
|
|
MYASTHENIA GRAVIS:
|
ETIOLOGY:
often associated with autoantibodies but not always autoantibodies bind to Ach receptors → blocking neuromuscular transmission to variable degree → inducing immune-mediated destruction of endplate → reducing number of functioning Ach receptors → weakness associated with HLA-DR3, hyperthyroidism, thymoma, RA, SLE GENETIC PREDISPOSITION: most common in young women with RISK FACTORS: most common in young women with HLA-DR3 most common in older men if thymoma is cause CLINICAL PRESENTATION: usually insidious onset but may be exacerbated by infection, before menstrual period, pregnancy, postpartum fluctuating weakness of commonly used voluntary muscles → cranial muscles (ocular, masticatory, facial, pharyngeal), respiratory, limb → ptosis, ocular palsies, diplopia, difficulty chewing or swallowing, respiratory difficulties, limb weakness sustained activity increases weakness of affected muscles but improves after brief rest sensation and DTRs normal symptoms fluctuate throughout day weakness may be localized or become generalized slowly progressive DIAGNOSTIC WORKUP: Ach receptor antibody assay AP and lateral CXR and CT to search for thymoma electromyography short-acting anticholinesterases transiently improve weakness COMPLICATIONS: myasthenia crisis → acute exacerbation, may lead to respiratory weakness requiring admission to ICU |
|
|
|
MULTIPLE SCLEROSIS:
|
ETIOLOGY:
probably autoimmune genetic components GENETIC PREDISPOSITION: HLA antigens (HLA-DR2) alleles IL2RA and IL7RA RISK FACTORS: usually <55y/o greatest incidence in young adults more common if western European lineage + living in temperate zone CLINICAL PRESENTATION: episodic neurologic symptoms single pathologic lesion can’t explain clinical findings initially presents as fatigue, weakness, numbness, tingling or unsteadiness in a limb; spastic paraparesis; retrobulbar optic neuritis; diplopia; disequilibrium; sphincter disturbance such as urinary urgency or hesitancy may be interval of months or years after initial episode before recurrent/new symptoms may be relapse-remission episodes or steady decline diagnosis requires involvement of different parts of the central nervous system at different times definitive diagnosis if relapsing-remitting course and evidence of ≥2 two lesions involving different regions of central white matter probable diagnosis if only 1 clinical attack + multiple white matter lesions or ≥2 clinical attacks + 1 white matter lesion DIAGNOSTIC WORKUP: MRI of brain or spinal cord to visualize multiple lesions → areas of demylelination scattered in white matter of brain and spinal cord COMPLICATIONS: some disability eventually but 50% of patients do not have significant disability 10 years after onset |
|
|
|
List the cranial nerves.
|
I olfactory
II optic III oculomotor IV trochlear V trigeminal VI abducens VII facial VIII vestibulocochlear IX glossopharyngeal X vagus XI accessory XII hypoglossal |
|
|
|
List the cranial nerves and their corresponding cranial exam components.
|
I olfactory → none
II optic → visual acuity → snellen, rosenbaum, fundoscopy III oculomotor → inspect for ptosis, EOMs, convergence; inspect pupillary size/shape, corneal light reflex, accomodation IV trochlear → superior oblique m. → EOMs, corneal light reflex V trigeminal → inspect face for muscle atrophy, deviation of jaw to one side, fasciculations; clench teeth, move jaw side to side; soft, sharp, dull VI abducens → laterla rectus m. → EOM, corneal light reflex VII facial → raise eyebrows, close eyes and resist opening, puff cheeks and resist popping, smile, show teeth VIII vestibulocochlear → gross hearing IX glossopharyngal → stick out tongue, stay ah, gag reflex X vagus XI accessory → testing sternocleidomastoid and trapezius XII hypoglossal → stick tongue out |
|
|
|
What are the layers of the meninges?
|
(skin)
(muscle) (periosteum) (skull) (epidural space) dura mater subdural space arachnoid mater subarachnoid space pia mater |
Mosbys p760
|
|
|
What arteries supply the brain?
|
two internal carotid arteries
two vertebral arteries → basilar artery |
Mosbys p761
|
|
|
What are the parts of the cerebrum?
|
cerebrum divides into 2 cerebral hemispheres that each contain frontal lobe, temporal lobe, parietal lobe, and occipital lobe
cerbral cortex = outer layer |
Mosbys p762
|
|
|
What is the function of the frontal lobe?
|
contain motor cortex associated with voluntary skeletal movement, fine repetitive motor movement, eye movement
|
Mosbys p762
|
|
|
What is the function of the parietal lobe?
|
processing sensory data → visual, auditory, olfactory, gustatory, and tactile sensation; propioception
|
Mosbys p762
|
|
|
What is the function of the temporal lobe?
|
perception and interpretation of sound, smell, taste, and balance
|
Mosbys p762
|
|
|
What is the function of the occipital lobe?
|
contains primary vision center → interpretation of visual data
|
Mosbys p762
|
|
|
What is the function of the cerebellum?
|
assists motor cortex of cerebrum in integration of voluntary movement; processes sensory data from eyes, ears, touch receptors, and musculoskeleton → altering muscle tone, equilibrium, and posture
|
Mosbys p762
|
|
|
What structures comprise the brainstem?
|
medulla oblongata, pons, midbrain, diencephalon
|
Mosbys p763
|
|
|
What is the brainstem?
|
pathway between cerebral cortex and spinal cord; contains nuclei of CNs
|
Mosbys p763
|
|
|
What are cranial nerves?
|
peripheral nerves that arise from the brain (not the spinal cord)
|
Mosbys p763
|
|
|
What is the function of the pituitary gland?
|
hormonal control of metabolism, vasoconstriction, growth, and lactation
|
Mosbys p764
|
|
|
What is the function of the hypothalamus?
|
processing of internal stimuli for ANS; maintains temperature control, water metabolism, body fluid osmolarity, feeding behavior, and neuroendocrine activity
|
Mosbys p764
|
|
|
What is the function of the epithalamus?
|
house pineal body
sexual development and behavior |
Mosbys p764
|
|
|
What is the function of the olfactory nerve (CN I)?
|
sensory → smell
|
|
|
|
What is the function of the optic nerve (CN II)?
|
sensory → vision
|
|
|
|
What is the function of the oculomotor nerve (CN III)?
|
motor → raise eyelids, most EOMs
parasympathetic → constrict pupils, alter lens shape |
|
|
|
What is the function of the trochlear nerve (CN IV)?
|
motor → EOM of the superior oblique muscle → eyes move medially and inferiorly
|
|
|
|
What is the function of the abducens nerve (CN VI)?
|
motor → EOM of the lateral rectus muscle → eyes move laterally
|
|
|
|
What is the function of the trigeminal nerve (CN V)?
|
motor → clench teeth, open jaw, mastication
sensory → sensation to facial skin, forehead, eyelids, lacrimal gland, conjunctiva, cornea, iris, ear, nose, nasal mucosa, mouth mucosa, teeth, tongue |
|
|
|
What is the function of the facial nerve (CN VII)?
|
motor → close eyelids, movement of facial expression muscles except jaw, labial speech sounds (b, m, w, and rounded vowel sounds)
sensory → taste (anterior 2/3rds of tongue), sensation to pharynx parasympathetic → secretion of tears and saliva |
|
|
|
What is the function of the vestibulocochlear nerve (CN VIII)?
|
sensory → hearing, balance
|
|
|
|
What is the function of the glossopharyngeal nerve (CN IX)?
|
motor → voluntary muscles for swallowing and phonation (gutteral speech sounds)
sensory → sensation of nasopharynx, taste (posterior 1/3rd), gag reflex parasympathetic → secretion of salivary glands , carotid reflex |
|
|
|
What is the function of the vagus nerve (CN X)?
|
sensory → sensation behind ear and part of external ear canal
parasympathetic → secretion of digestive enzymes, peristalsis, carotid reflex, involuntary action of heart, lungs, and GI tract |
|
|
|
What is the function of the function of the acessory nerve (CN XI)?
|
motor → turn head, shrug shoulders, some phonation
|
|
|
|
What is the function of the hypoglossal nerve (CN XII)?
|
motor → tongue movement for sound articulation (l, t, d, n), swallowing
|
|
|
|
Describe the neurological exam.
|
Cerebral Function:
1. check altertness and orientation → document as A&O x 4 -name -date → day, month, year, season -place -purpose 2. test memory -recent memory → ask patient to remember 3 simple words, ask to repeat, then ask to repeat later on in exam → ball, cat, apple -remote memory → ask president 3. test graphesthesia → ask patient to close eyes, draw letter in hand, bilaterally 4. test stereognosis → ask patient to keep eyes closed, place object in hand, use different object for other hand 5. ask patient to recall words Cerebellar Function 1. finger-nose touch → eyes open, faster, moving, eyes closed, bilaterally 2. rapid alternating movements -upper extremities -lower extremities 3. shin-scrape |
|
|
|
Define graphesthesia.
|
ability to recognized writing on the skin by the sensation of touch
|
|
|
|
List the deep tendon reflexes and the associated spinal roots being tested.
|
biceps→ C5
brachioradialis → C6 triceps → C7 patellar → L4 achilles → S1, S2 |
|
|
|
Describe the grading scale for tendon reflexes.
|
0 = absent
1+ = trace 2+ = normal 3+ = hyperactive without clonus 4+ = hyperactive with clonus |
|
|
|
List the superficial reflexes and the associated spinal roots being tested.
|
abdominal →
cremasteric → plantar → |
|
|
|
Define anosmia.
|
loss of sense of smell or inability to discriminate odors
|
Mosbys p776
|
|
|
What is the ddx for anosmia?
|
trauma to cribiform plate
olfactory tract lesion |
Mosbys p776
|
|
|
What is the ddx for reduced sense of smell?
|
inflammation of mucous membranes
allergic rhinitis smoking |
Mosbys p776
|
|
|
How is normal alertness and orientation documented?
|
A&O x 4
|
|
|
|
How are normal pupils documented?
|
PERRLA
|
|
|
|
If patient complains of severe constant headaches, what should you look for?
|
impaired extraocular movement in lateral direction → suggests impaired lateral rectus muscle → suggests impaired abducens nerve
*abducens nerve usually loses function first in presence of increased ICP |
Mosbys p777
|
|
|
Which cranial nerve usually loses function first with increased ICP?
|
abducens (CN VI) → loss visible when evaluting lateral rectus muscle (EOMs impaired in lateral direction)
|
Mosbys p777
|
|
|
How do you perform the corneal reflex test?
|
1. if present, ask patient to remove contact lenses
2. ask patient to look up and away 3. approach patient from side 4. touch cornea with cotton, avoiding eyelashes and conjunctiva 5. if corneal reflex present, patient should blink bilaterally |
Mosbys p777
|
|
|
What is the ddx for absent corneal reflex?
|
use of contact lenses (may be diminished or absent)
damage to opthalmic branch (V1) of trigeminal nerve (CN V) |
Mosbys p777
|
|
|
How do you evaluate nasopharyngeal sensation?
|
gag reflex → palate should move upward, pharnygeal muscles should contraction, uvula should remain midline
|
Mosbys p778
|
|
|
What cranial nerves are responsible for nasopharyngeal sensation?
|
glossopharyngeal
vagus |
Mosbys p778
|
|
|
Failure of palate to rise + deviation of uvula from midline may indicate?
|
glossopharyngeal or vagus nerve damage
|
Mosbys p778
|
|
|
Deviation of tongue from midline may indicate?
|
hypoglossal nerve damage
|
Mosbys p779
|
|
|
What is past pointing?
|
occurs during finger-nose test
patient consistently misses touching examiners finger may indicate cerebellar disease |
Mosbys p781
|
|
|
Past pointing may indicate?
|
cerebellar disease
|
Mosbys p781
|
|
|
Define ataxia.
|
gross lack of muscle coordination
|
|
|
|
What is the ddx for positive Romberg sign (i.e. loss of balance)?
|
cerebellar ataxia
vestibular dysfunction sensory loss |
Mosbys p781
|
|
|
What evaluating gait, what are you looking for?
|
normally smooth, symmetric with regular rhythm
shuffling, widely placed feet, walking on toes, drop foot, leg lag, scissoring, loss of arm swing, staggering, reeling |
Mosbys p783
|
|
|
Deviation of the tongue to the left may indicate?
|
left hypoglossal (CN XII) palsy
|
|
|
|
Define stereognosis.
|
ability to recognize an object by touch
|
|
|
|
What must you remember when evaluating a musculoskeletal complaint?
|
1. examine joint above and below complaint
2. examine contralateral side |
|
|
|
Define gait cycle.
|
interval from heelstike to heelstrike of same foot
|
|
|
|
What percentages do the stance and swing phases comprise of the gait cycle?
|
stance = 60%
swing = 40% |
|
|
|
Where is the visual cortex located?
|
near calcarine sulcus of occipital lobe of cerebral cortex
|
|
|
|
The primary visual cortex receives info from?
|
ipsilateral lateral geniculate nucleus (LGN)
|
|
|
|
List the EOMs involved in eye movement.
|
CN III, IV, V
|
|
|
|
What CN is involved in focusing the lens of the eye?
|
CN III (visceral motor)
|
|
|
|
What CN is involved in constricting the pupil?
|
CN III (visceral motor)
|
|
|
|
What CN is involved in raising the eyelids?
|
CN III (somatic motor)
|
|
|
|
Where is the center for lateral gaze located?
|
paramedian pontine reticular formation (PPRF) of pons
|
|
|
|
Is pupillary constriction controlled by the parasympathetic or sympathetic nervous system?
|
parasympathetic
|
|
|
|
Is pupillary dilation controlled by the parasympathetic or sympathetic nervous system?
|
sympathetic
|
|
|
|
Is lens thickening and near vision controlled by the parasympathetic or sympathetic nervous system?
|
parasympathetic
|
|
|
|
Paralysis of lower half of face indicates?
|
UMN lesion (lesion to primary motor cortex)
think stroke!!! weakness in contralateral lower half of face |
|
|
|
Paralysis of entire half of face indicates?
|
LMN lesion (lesion to nerve)
think bell's palsy!!! weakness in contralateral upper and lower halve of face |
|
|
|
What are UMNs?
|
motor neurons that originate in the cerebrum and terminate in the brainstem or spinal cord
|
|
|
|
What are LMNs?
|
motor neurons that originate in the brainstem (cranial nerves) or spinal cord (spinal nerves) and terminate at the neuromuscular junction (muscles)
|
|
|
|
Are descending motor pathways found in the ventral horn or the dorsal horn?
|
ventral
|
|
|
|
Are ascending sensory pathways found in the ventral horn or the dorsal horn?
|
dorsal
|
|
|
|
Posterior spinal artery infarct causes?
|
effects ipsilateral DCML
causing ipsilateral loss of proprioception and vibratory sensation |
|
|
|
List LMN signs.
|
weakness
hypotonia hyporeflexia marked muscle atrophy fasciculations flaccid paresis (or paralysis) |
|
|
|
List UMN signs.
|
weakness
hypertonia hyperreflexia Babinski disuses muscle atrophy spastic rigidity |
|
|
|
What is the corticospinal tract?
|
descending motor pathway
collection of axons that travel between the cerebral cortex and the spinal cord fibers separate into: lateral corticospinal tract anterior corticospinal tract |
|
|
|
Anterior cerebral artery supplies blood to?
|
medial frontal lobes
superior medial parietal lobes |
|
|
|
Anterior cerebral artery infarct manifests as?
|
contralateral UMN signs
weakness in contralateral leg somatosensory deficits in contralateral leg no visual, auditory, or language deficits *legs are most medial (think FATL) |
|
|
|
Posterior cerebral artery supplies blood to?
|
occipital lobes
|
|
|
|
Posterior cerebral artery infarct manifests as?
|
contralateral homonymous hemianopsia
no motor, somatosensory, auditory, or language deficits |
|
|
|
Middle cerebral artery supplies?
|
lateral cerebral cortex
anterior temporal lobes insular lobes |
|
|
|
Middle cerebral artery infarction manifests as?
|
ipsilateral somatosensory deficits (entire face, upper limb, maybe lower limb)
ipsilateral motor deficits (lower face, upper limb > lower limb) language deficits (if RT handed + LT MCA infarct then global aphasia; if RT handed + RT MCA infarct then aprosody i.e. lack of variation in speed tone inflexion no visual or auditory deficits (getting info from both ears) |
|
|
|
Lesions in the RT primary visual cortex manifest as?
|
LT homonymous hemianopia with macular sparing
|
|
|
|
What are the watershed stroke?
|
stroke affecting areas of brain farthest away from direct perfusion by major cerebral arteries
d/t hypoperfusion (ex: hypotension, CHF, atherosclerosis of carotid arteries |
|
|
|
What is a watershed area?
|
region that receives blood supply from the distal branches of 2 large arteries
*if atherosclerosis occurs, region is spared from ischemia d/t dual blood supply *if hypoperfusion occurs, region is particularly vunerable |
|
|
|
Deficits affecting one side of face and opposite side of body indicates?
|
unilateral damage to brainstem
|
|
|
|
Posterior spinal artery infarct manifests as?
|
effects DCML
ipsilateral proprioception deficit |
|
|
|
Posterior inferior cerebral artery infarct manifests as?
|
infarct of lateral medulla
ipsilateral deficit in pain/temp for face (trigeminal nucleus) ipsilateral hearing loss (cochlear nucleus) vertigo, nystagmus (drift to impaired side and beat back to contralateral side), leaning to ipsilateral side (vestibular nucleus) contralateral deficit of pain/temp for body |
|
|
|
Where is the primary visual cortex located?
|
occipital lobe
|
|
|
|
A lesion or infarct in primary visual cortex manifests as?
|
homonymous hemianopsia with macular sparing
|
|
|
|
What are the reversible causes of dementia?
|
neurosyphilis
B12 deficiency hypothyroidism normal pressure hydrocephalus intercranial mass lesion |
|
|
|
What is pseudodementia?
|
depression
|
|
|
|
What is normal pressure hydrocephalus?
|
abnormal accumulation of CSF in ventricles - increased ICP - ICP eventually falls back to normal but ventricles enlarge putting pressure on adjacent cortical tissue - resulting in dementia, urinary incontinence and gait disturbance
|
|