Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
97 Cards in this Set
- Front
- Back
- 3rd side (hint)

Lowenstein-Jensen medium
|
dry, heaped-up yellow to buff-colored colonies of Mycobacterium tuberculosis.
|
|
|

|
M marinum is characterized by broad bacilli with cross banding.
|
|
|

|
Escherichia coli : Good growth, green metallic sheen.
Klebsiella pneumoniae : Good growth, purple colonies, no sheen. Shigella flexneri : Good growth, transparent colonies (lactose negative) |
|
|
|
Lowenstein-Jensen agar , rapid grower, arylsulfatase +, nitrate+
|
M. fortuitum
|
|
|
|
Lowenstein-Jensen agar , rapid grower, arylsulfatase +, nitrate=
|
M. chelonae
|
|
|
|
Lowenstein-Jensen agar , niacin+
|
M. tuberculosis
|
|
|
|
Lowenstein-Jensen agar , niacin=
|
MAI (( resemble whipple disease)), M.bovis
|
|
|
|
M. abscessus
M. chelonae M. fortuitum |
Rapidly Growing Mycobacteria
|
|
|
list the other photos?
|
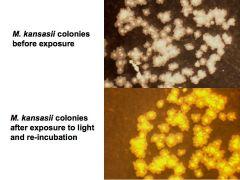
Group I - photochromogens, develop yellow or orange pigment when exposed to light;
Mycobacterium marinum, Mycobacterium asiaticum Mycobacterium kansasii, Mycobacterium simiae. |
|
|

other scotos?
|
Group II - scotochromogens, form orange-yellow pigment in the dark;
Mycobacterium gordonae, Mycobacterium szulgai Mycobacterium scrofulaceum |
|
|
|
scoto at 37C
photo at room temp 22C |
Mycobacterium szulgai
|
|
|
|
M. malmoense
M. avium complex (MAC) M. xenopi |
Group III - nonchromogens, are unpigmented
|
|
|
|
M. chelonae
M. abscessus M. fortuitum |
Group IV - rapid growers
|
|
|
|
3rd leading cause of blindness worldwide
|
M.leprae(Hansen disease); in US - HAWAII,TEXAS,LOUSIANA; armadillos
|
|
|
|
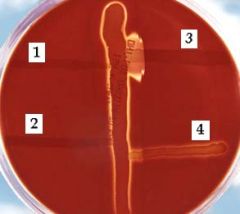
The vertical streak is a beta-hemolysin-producing strain of Staphylococcus aureus, and at right angles to it are streaks of (1)Enterococcus faecalis, (2)Streptococcus salivarius, (3)S. agalactiae, and (4)E. durans. Note the large area of complete lysis where the extracellular compound of S. agalactiae encounters the beta-lysin of S. aureus.
|
|
|

Catalase positive reaction
|
S. aureus infection
|
|
|
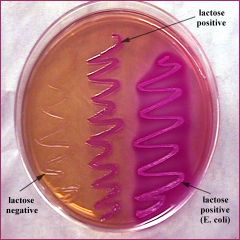
MacConkey agar
|
Red colonies: Escherichia, Klebsiella, Enterobacter (strong lactose fermenters)
Pink colonies: Citrobacter, Providencia, Serratia, Hafnia Colorless colonies: Proteus, Edwardsiella, Salmonella, Shigella |
|
|
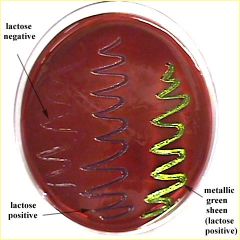
Eosin methylene blue (EMB) agar
|
Green-black-purple colonies: Escherichia, Klebsiella, Enterobacter, Serratia, Hafnia, Citrobacter, Providencia
Colorless colonies: Proteus, Edwardsiella, Salmonella, Shigella |
|
|

|
Triple Sugar Iron agar slant (TSI slant)
Escherichia coli : A/A (G) (+lactose) Shigella flexneri : K/A (+glucose,-lactose) Proteus vugaris : K/A, H2S (+glucose,-lactose, +H2S) Pseudomonas aeruginosa : K/N |
K = alkaline = Red; A = acid = Yellow; NC = No change; G = gas produced; H2S = hydrogen sulfide produced
|
|
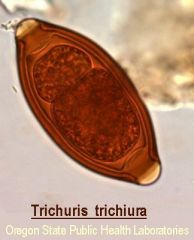
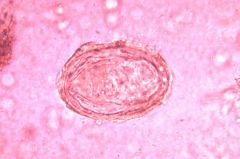
nematode
|
infection via ingestion of eggs; heavy infestations=rectal prolapse in young kids; dual infection with Ascaris lumbricoides
|
|
|

trematode
|
schistosoma mansoni
Africa, Nile delta infect hepatic portal vasculature and inferior mesenteric vessels pipestem fibrosis----cirrrhosis |
|
|
trematode
|
schistosoma japonicum
Philippines,China, SE asia infect the liver |
|
|

trematode
|
Schistosoma haematobium
Africa , Middle east infect veins of bladder long term=squamous cell ca. of bladder detected in terminal urine specimen, midday;S.INTERCALATUM INTESTINE |
|
|

trematode
|
Fasciola hepatica
large ingestion feshwater plants infestation of bile ducts with eventual biliary fibrosis |
|
|

|
Chinese liver fluke, or oriental liver fluke
ingestion of undercooked freshwater fish; biliary fibrosis; cholangiocarcinoma clonochis sinensis |
|
|

|
Chinese liver fluke, or oriental liver fluke
ingestion of undercooked freshwater fish; biliary fibrosis; cholangiocarcinoma |
|
|
Regan Lowe Charcoal agar
|
Bordetella pertussis
PCR useful for partially treated cases detect or confirm with FA stain |
|
|
|
Mueller Hinton II Broth with Lysed Horse Blood is for use
in broth dilution antimicrobial susceptibility testing of |
Streptococcus
pneumoniae with 11 antimicrobial agents |
|
|
dimorphic
|
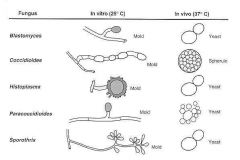
H. capsulatum
granuloma/necrotizing organism within histiocytes |
|
|
|
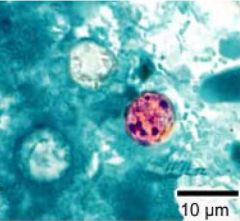
Cyclospora cayetanensisGastroenteritis
|
|
|
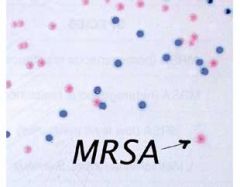
CHROM agar
|
Methicillin Resistant Staphylococcus aureus - mauve
Other bacterial colonies - inhibited, blue or colourless |
|
|

|
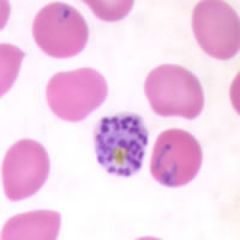
A: Stages of P. falciparum in thin blood smears. Fig. 1: Normal red cell; Figs. 2-18: Trophozoites (among these, Figs. 2-10 correspond to ring-stage trophozoites); Figs. 19-26: Schizonts (Fig. 26 is a ruptured schizont); Figs.27, 28: Mature macrogametocytes (female); Figs. 29, 30: Mature microgametocytes (male).
|
|
|

|
Ring-form trophozoites of P. falciparum in a thin blood smear.
|
|
|
|
Ring-form trophozoites in a thin blood smear, exhibiting Maurer's clefts./falciparum
|
|
|
|
Schizont of P. falciparum in a thin blood smear.
|
|
|
|
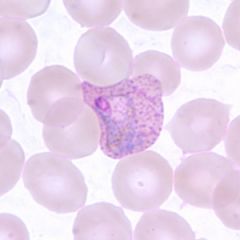
Trophozoites of P. vivax in a thin blood smear. Note the amoeboid appearance and Schüffner's dots.
|
|
|
|
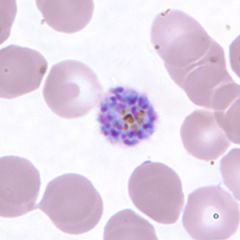
schizont of P. vivax in a thin blood smear.
|
|
|
|
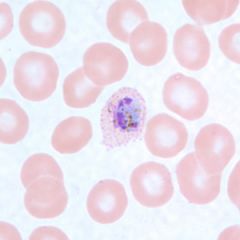
Trophozoites of P. ovale in thin blood smears. Note the fimbriation and Schüffner's dots.
|
|
|

|
Enterobius vermicularis
The incidence of D. fragilis is nine times higher in patients with pinworm infections, suggesting that E. vermicularis eggs may be infected with the flagellate and serve as the chief vector for transfer to humans. |
|
|

The parasite egg in image 1 was identified. What parasite has a high incidence of being found in association with
the one in the image? a) Isospora belli b) Entamoeba histolytica c) Giardia lamblia d) Dientamoeba fragilis |
d is correct. The parasite egg in the image is that of Enterobius vermicularis. Note the shape resembling a
football, the smooth, thin wall, and the absence of opercula. The incidence of D. fragilis is nine times higher in patients with pinworm infections, suggesting that E. vermicularis eggs may be infected with the flagellate and serve as the chief vector for transfer to humans. |
|
|

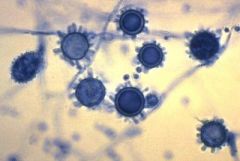
The organism in image 2 (Sabouraud dextrose plate) was cultured from lung tissue obtained from an organ
transplant patient. What is the organism? a) Mucor spp. b) Histoplasma capsulatum c) Aspergillus fumigatus d) Aspergillus terreus |
c is correct. The image is that of a mold with a central blue-green zone and a
white peripheral apron which is characteristic of A. fumigatus. The other choices don't have this characteristic appearance. Mucor spp. (choice a) grows rapidly so that it will quickly cover the entire surface of the plate and may lift the lid of the plate. H. capsulatum (choice b) usually appears as delicate cobweblike, gray-white mycelium. A. terreus (choice d) has some sort of yellow or brown pigmentation. |
|
|
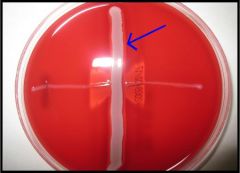
Image 4 is that of a test used to presumptively identify a catalase-negative streptococcus with characteristic
hemolysis. Which organism is streaked perpendicular (identified by arrow) to the presumptive organism (presumptive - the unknown organism being tested)? a) S. aureus b) Group A Streptococcus (S. pyogenes) c) Group D Streptococcus d) Enterococcus spp. |
a is correct. The image is that of the CAMP test used to identify group B streptococcus. S. aureus is streaked
along almost the entire diameter of the blood agar plate, and the presumptive GBS is streaked perpendicular to this. Most strains of S. aureus produce a β-hemolysin. These β-hemolysins diffuse out into the agar, and the extracellular protein produced by GBS (CAMP factor) diffuses out into the agar. Where these two substances intersect, you observe synergistic hemolysis. |
|
|
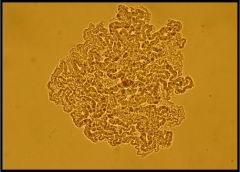
The organism seen in image 5 is that of mycobacterium growing on a plate. Which of following mycobacteria show
this morphology? a) M. simiae b) M. marinum c) M. szulgai d) M. tuberculosis |
d is correct. The mycobacterium in the image is showing cording. Of the choices, only M. tuberculosis can
have this appearance, which is due to production of "cording factor." As a matter of fact, all the organisms of the MTB complex can have this appearance. |
|
|
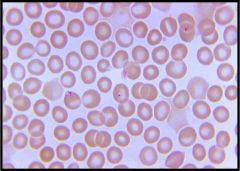
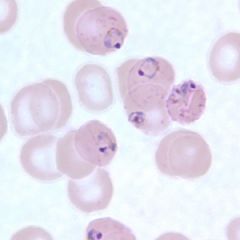
See image 6 of a peripheral blood smear. You obtain the history that this patient lives on the Northeast Coast with
her family, and none of them have strayed far from that area. She recently developed fever, malaise, anorexia, and fatigue. What is the most likely diagnosis? a) Ehrlichia chaffeensis b) Babesia microti c) Plasmodium falciparum d) Borrelia recurrentis |
b is correct. It may be very difficult to distinguish B. microti from the early ring forms of P. falciparum on a
peripheral smear if the characteristic Maltese cross (indicating the mature form of B. microti) is not identified. While P. falciparum (choice c) is certainly a consideration, the fact that this patient hasn't really travelled makes it less likely. Neither E. chaffeensis (choice a) nor B. recurrentis (choice d) infect red blood cells. With E. chaffeensis, a rickettsia-like bacteria, you see organisms (morula) in the cytoplasm of macrophages. B. recurrentis, the cause of relapsing fever, is a spirochete that, if seen in blood, is present outside of the red blood cells. |
|
|
|
Mycobacterium szulgai has an interesting characteristic. The organism is a _____ @ 25°C and a _____ @ 37°C.
a) non-photochromagen; photochromagen b) photochromagen; non-photochromagen c) scotochromagen; photochromagen d) photochromagen; scotochromagen |
d is correct. In the Runyon Classification Scheme, M. szulgai is classified as a scotochromagen (at 37°C).
Scotochromagens produce pigment in the dark and in the light. Photochromagens produce pigment only in the light and not in the dark. |
|
|
|
You get a call from a clinician who insists on ordering a “Legionella pneumophila antigen” on a urine specimen
because the team highly suspects this organism, has already started the patient on treatment, and would like to rapidly confirm their clinical diagnosis; however, you find out that no other microbiology test was ordered. What do you tell the clinician? a) The urine antigen test is a tedious test that takes several days to perform. Same-day results are not possible. Culture should also be considered. b) The Legionella pneumophila antigen test only detects serogroup 1. A negative urine antigen test does not mean that the patient does not have Legionella. Culture should also be considered. c) The results of the urine antigen test are affected by therapy; therefore, since the patient has already started treatment, a negative result does not necessarily mean the patient did not have Legionella. Culture should also be considered. d) The urine antigen test is not really a specific test. There is a lot of cross-positivity with Streptococcus pneumoniae in patients who are bacteremic. Culture should also be considered. |
Choice b is correct. The Legionella pneumophila antigen test only detects serogroup 1.
|
|
|
|
What obvious morphologic characteristic distinguishes Bacillus anthracis from Bacillus cereus?
a) B. anthracis is non-motile. b) B. cereus is non-motile. c) The spores of B. anthracis are present on the terminal ends of the organism. d) The spores of B. cereus are present on the terminal ends of the organism. |
Choice a is correct. The Bacillus genera are spore-forming, gram positive rods. Most of these organisms are motile
(choice b incorrect), with one notable exception being Bacillus anthracis. Neither B. anthracis nor B. cereus has spore present at the terminal ends of the organism (choices c and d). The spores are either subterminal (B. anthracis) or subterminal or central (B. cereus). |
|
|
|
Which of the following viruses are non-enveloped?
a) Parvovirus b) Hepatitis A c) Papovavirus d) all of the above |
Choice d is correct. Parvovirus and Papovavirus (choice a and c) are DNA viruses while hepatitis A (choice b) is an
RNA virus |
|
|
|
Which of the following features are associated with lepromatous leprosy?
widespread skin infections superinfection with Strongyloides non-caseating granulomas with few AFB A & B A, B, C |
D. A & B.
Lepromatous leprosy is associated with anergy and therefore a more widespread involvement with the presence of large numbers of acid-fast bacilli and foamy macrophages. The tuberculoid form is associated with a robust granulomatous reaction to infection. In tuberculoid form, there is a small number of organisms present. Two leprosy factoids: Mycobacterium leprae grows on armadillo footpads and the most consistent signs are anesthetic skin lesions with palpable prominent peripheral nerves. |
|
|
|
Which of the following mycobacterial species is the cause of the Buruli ulcer?
M. leprae M. ulcerans M. fortuitum M. marinum M. chelonei |
B. M.
The necrotizing ulcerative cutaneous Buruli ulcer is caused by infection with M. ulcerans. All the choices are notable for causing skin disease without pulmonary disease. Most are associated with penetrating trauma - M. marinum with fresh water fish tanks. |
|
|
|
What condition particularly predisposes toward M. kansasii pulmonary disease?
pneumoconiosis pre-existing M. tuberculosis squamous cell carcinoma of the lung diabetes mellitus congenital pulmonary adenomatoid malformation |
A. PNEUMOCONIOSIS.
Behind Mybacterium tuberculosis and M. avium-intracellulare, M. kansasii is one of the most common causes of mycobacterial pulmonary disease. |
|
|
|
Which of the following coinfections often lead to smear-negative TB and PPD anergic false-negative results?
HCV Borrelia burgdorfei Ascaris lumbricoides HIV methicillin-resistant Staphylococcus aureus |
D. HIV.
TB is a difficult disease to diagnose - screening tests like PPC and sputum smears have high false-negative rates and culture often takes weeks. Nucleic acid amplification tests may be more sensitive and rapid, but long-term validation is lacking. HIV makes diagnosis even more difficult. |
|
|
|
What percentage of immunocompetent people infected with primary TB infection develop active TB?
0% 10% 50% 90% 100% |
B. 10%.
Actually, 10% is on the high side of estimates as the vast majority of people (90%) infected with respiratory TB resolve the infection. The remaining 5-10% (higher in the immunocompromised) go on to develop active disease, which most often is pulmonary, but can also be extrapulmonary. QCCP2, M. tuberculosis |
|
|
|
Staphylococci
Streptococci Enterococcus |
Gram + cocci
|
|
|
|
Bacillus
Clostridium Corynebacterium Listeria Actinomyces Nocardia Mycobacterium |
Gram + bacilli
|
|
|
|
Mycoplasma
Ureaplasma |
Mycoplasma
|
|
|
|
Neisseria
Moraxella |
Gram -- cocci
|
|
|
|
Pseudomonas
Legionella Boertella Francisella Brucella |
Gram -- bacilli (AEROBIC)
|
|
|
|
Campylobacter
Helicobacter |
Gram -- curved bacteria (Microaerophilic)
|
|
|
|
Escherichia
Klebsiella Shigella Salmonella Proteus Yersinia |
Gram -- bacilli (anAerobic, facultative)
|
|
|
|
Citrobacter
Enterobacter Escherichia Klebsiella |
C E E K
lactose fermenters; enterobacteriacae |
|
|
|
Shigella
Yersinia Proteus Salmonella ShY: nonmotile, no H2S PS : motile; yes H2S |
Sh Y P S
lactose nonfermenter enterobacteriacae |
|
|
|
All ferment glucose,
oxidase negative, catalase positive reduce nitrates to nitrites |
Enterobacteriaceae
|
|
|
|
Vibro
Haemophilus Pasteurella |
Gram -- bacilli (anAEROBIC, facultative)
non-Enterobacteriaceae |
|
|
|
Treponema
Borrelia Leptospira |
Gram --- envelope, spirochetes)
|
|
|
|
VDRL( venereal disease research laboratory test)
RPR( rapid plasma reagin test) ART (automated reagin test) |
Nontreponemal (reaginic) tests;
Appears one week later, non specific, may also be positive in autoimmune disease....lupus, viral hepatitis |
|
|
|
FTAB-ABS (fluorescent treponemal antibody absorption test)
MHA-TP (microhemagglutination-Treponema pallidum) |
Treponemal Ab test
used to confirm; specific |
|
|
|
Rickettsia
Ehrlichia Bartenella Coxiella |
Rickettsiaceae
|
|
|
|
Chlamydiae
|
Obligate intracellular bacteria
|
|
|

|
Staph epidermidis:endocarditis
Staph saprophyticus: UTI |
|
|
|
Bile esculin - positive
6.5% NaCl - negative(Enterococcus = +) PYR - negative . When found in blood associated with Bowel carcinoma. Increased % in bowel due to higher levels of bile or underlying colonic disease . Always susceptible to Penicillinbcd5c8 |
Streptococcus Group D not
enterococcus Streptococcus bovis |
|
|
|
A urine specimen from a middle aged female is received in the lab and grows small white colonies on sheep blood
agar that are coagulase negative and positive for catalase. The Gram stain reveals Gram-positive cocci in clusters. The organism is plated onto a Mueller-Hinton agar and a Novobiocin disc is placed onto the plate. The next morning, the plate is examined and shows no zone of inhibition. What is the MOST LIKELY organism growing on this plate? a. Staphylococcus epidermidis b. Staphylococcus aureus c. Staphylococcus saprophyticus d. Staphylococcus lugdunensis e. Staphylococcus haemolyticus |
C. Many of the different species of Staphylococcus can be differentiated by simple testing. The coagulase
negative Staphylococcus organisms include S. epidermidis and S. saprophyticus. While both organisms are catalase positive, differentiation can be made using Novobiocin. S. saprophyticus is resistant while S. epidermidis is sensitive½Ò¬u |
|
|
|
You receive plates from a respiratory specimen that exhibit no growth on a blood agar plate and growth of small
gray colonies on a chocolate plate. You perform a gram stain, which reveals small, pleomorphic gram-negative rods. Based on these results you conclude that this organism is a Haemophilus species. To further subtype the organism, you test for factor requirements and hemolysis. The next day, you examine the plate and based on the growth, you determine the organism is H. influenzae. What growth pattern most closely resembles the expected findings for this organism? a. Growth and hemolysis, does not require factor X, does not require factor V b. Growth and hemolysis, requires both factors X and V c. Growth and hemolysis, does not require factor X, requires factor V d. Growth but no hemolysis, requires both factors X and V e. Growth but no hemolysis, does not require factor X, requires factor V |
D. Haemophilus influenza type b is one of the leading causes of bacterial meningitis worldwide, especially in
young unvaccinated children. Infection with Haemophilus can also cause cellulitis, pericarditis and pneumonia. Pneumonia is typically caused by non-type b strains, most commonly serotype f. Haemophilus is a gram negative rod. Differentiating species can be accomplished by testing for factor requirements and observing hemolysis. All Haemophilus species isolated from humans require factor V. H. influenzae does not show hemolysis on blood agar and requires factor X. An alternate method for testing for factor X requirement is the porphyrin test. In addition, Haemophilus is one of the few organisms that show satellite growth around a streak of Staphylococcus aureus.or V |
|
|
|
In preparation for an upcoming laboratory inspection, you are reviewing your quality control procedures in the
microbiology department. You have a list of atypical bacteria-antibiotic resistance profiles that are posted and should alert the technicians to perform confirmatory testing. Which of the following bacteria-antibiotic resistance combinations is INCORRECT and should prompt retesting by another method to confirm resistance? a. Proteus resistant to cefazolin b. Klebsiella resistant to ampicillin c. Enterobacter resistant to ampicillin and cefazolin d. E. coli resistant to no antibiotics e. Serratia resistant to ampicillin, cefazolin and cefuroxime |
A. Strains of Proteus are resistant to nitrofurantoin but are susceptible to the remainder of the drugs that are
commonly tested. The other microorganism-drug combinations are expected patterns of resistance. |
|
|
|
Which spiral bacterium has hooks at both ends?
a. Leptospira b. Borrelia c. Treponema d. Brachyspira e. Helicobacter¬«4 |
A. All of the choices are spiral bacteria, but only Leptospira has hooked ends. Leptospira is a tightly coiled,
right-hand spiraled bacteria. Infection of humans occurs most commonly via direct contact with infected animals through cuts on the skin or via the conjunctiva. Most infections have a mild clinical course and resolve while recognized infections present with sudden onset of fever, chills and myalgia. The minority of cases present with jaundice, acute renal failure, pulmonary hemorrhage and cardiac arrhythmias, known as Weil's disease. |
|
|
|
You finalize a report from a skin wound as no growth after 5 days. The clinician calls and he is concerned that the
specimen was not cultured correctly, as he was certain there was adequate material upon collection. He states that the patient had an abscess on the thigh and upon drainage, there was 25ml of purulent fluid expressed from the lesion. Following the drainage, a swab culture was taken for microbiology. The clinician sent the swab for gram stain, aerobic and anaerobic cultures. Your BEST response to address the clinician's concern is: a. Occasionally organisms just do not grow and we cannot explain why. Ask the clinician to send another swab and the lab will repeat the cultures. b. A swab should only be used if no other type of specimen can be submitted and in that case, one swab should be submitted for each type of culture c. Swabs never contain adequate material and should not be used for culturing specimens in the microbiology laboratory d. Occasionally organisms just do not culture and we cannot explain why. Tell the clinician you will reculture the specimen from the original swab e. Tell the clinician you will allow the plates to incubate for another 3 days to see if there will be delayed growth and then issue an amended report at that timeBntãBnt |
B. Preferred specimens for microbiologic culture include fresh tissue, fluid, exudates and instrumentation (i.e.
screws, plates, catheter tips). A specimen should be submitted to microbiology on a swab only when there is no availability of other types of specimens. Material submitted on a swab often yields an inadequate amount of material for culture. To increase the likelihood of having enough material for culture on a swab, one swab should be submitted for each type of culture the clinician desires. For example, one swab should be submitted for each of the following: Gram stain, aerobic culture and anaerobic culture, for a total of three swabs.cefur |
|
|
|
You receive a respiratory specimen in the laboratory that is labeled bronchial washing and has been obtained by
bronchoscopy. As standard procedure in your lab, you culture the specimen to a blood and buffered charcoal yeast extract plate. On the third day, you examine the plates and notice colonies growing that you would describe as having a ground-glass appearance. You perform a Gram stain and see tiny gram-negative rods. There is no growth on the blood plate. What is the MOST LIKELY organism growing on the BCYE plate? a. Neisseria gonorrhoeae b. Mycoplasma pneumoniae c. Moraxella catarrhalis d. Burkholderia cepacia e. Legionella pneumophiliafur |
E. Legionella is a fastidious, slow growing organism. Buffered charcoal yeast extract should be used to allow
for the growth of the Legionella organism. The cultures must be observed for 7 days due to the slow rate of growth of this organism. L. pneumophilia is the most common organism and colonies have a ground-glass appearance with iridescent edges. Gram stain of the organism reveals tiny gram-negative rods. Hospital acquired Legionella most often originates in the water distribution system and environmental studies should be performed in these cases.copla |
|
|

You receive a proficiency test unknown in your microbiology lab. You are told the specimen is from a wound, so you
plate the specimen onto your four standard agars. Pictured are the colonies on MacConkey agar. Based on these findings, you perform an indole test and find that it is positive. What is the MOST LIKELY organism? a. Citrobacter freundii b. Klebsiella pneumoniae c. Pseudomonas aeruginosa d. Klebsiella oxytoca e. Proteus |
D. The colonies pictured are growing on MacConkey agar and are pink, which indicates that they are lactose
positive. Of the choices, only the Klebsiella and C. freundii are lactose positive. The colonies are mucoid, which is most characteristic of Klebsiella species due to their capsule. Differentiation between K. pneumoniae and K. oxytoca can be made by testing for indole. K. pneumoniae is negative for indole while K. oxytoca is positive. Klebsiella are gramnegative rods carried in the nasopharynx and the bowel and are a frequent cause of urinary tract infections. |
|
|

You isolate a Staphylococcus aureus on a specimen from a wound. You test for Erythromycin susceptibility and find
that the organism is resistant. You perform a D-test disk diffusion test to evaluate clindamycin inducible resistance. Based on the results pictured, can you treat this patientʼs infection with clindamycin? a. No. The discs are too close together and therefore the test is not valid b. No. The zone of resistance around the clindamycin disc indicates that the bacteria is resistant to clindamycin c. No. Because there is no zone of inhibition around the erythromycin disc, the test is not applicable d. No. The flattening of the clindimycin zone of inhibition near the erythromycin disc indicates the organism is resistant to clindamycin e. Yes. The size of the zone of inhibition surrounding the clindamycin disc indicates that the bacteria is susceptible to clindamycin |
D. D Zone Test for Inducible Clindamycin Resistance in Methicillin Resistant Staphylococcus Aureus (MRSA)Clindamycin is an excellent antibiotic for the treatment of methicillin sensitive Staphylococcal infections. For the test to
be valid, there must be a zone of inhibition around the clindamycin and no zone around the erythromycin. For the test to be positive, inferring that the organism is resistant to clindamycin, there must be flattening of the zone of inhibition around the clindamycin, nearest the erythromycin disc. |
|
|

You receive a cultured specimen on a MacConkey plate. Based on the growth pictured, you perform an oxidase
test, which is positive. What is the BEST organism identification for this specimen? a. Proteus mirabalis b. Enterobacter cloacae c. Pseudomonas aeruginosa d. Klebsiella pneumoniae e. Escherichia coli |
C. Based on the picture, the organism growing on the plate is lactose negative. Of the choices, the only
organisms that fall into this category are Pseudomonas and Proteus. Differentiation can be made by an oxidase test, which is positive with Pseudomonas and negative with Proteus. Pseudomonas is a Gram-negative rod that is slightly curved and has one or more flagella. The organisms are lactose non-fermenters on MacConkey agar, oxidase positive and catalase positive. Pseudomonas aeruginosa is known to cause folliculitis in association with swimming pools and whirlpools, “swimmers ear”, as well as infections in patients with cystic fibrosis. |
|
|
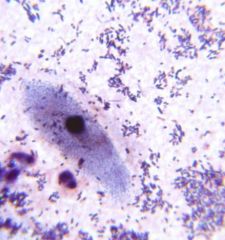
A clinician calls for a preliminary report on a wound specimen. As the resident on microbiology, you are asked to
review the Gram stain made from the specimen. Based on the image, what is the MOST APPROPRIATE interpretation of this stain? a. Gram positive rods in chains are present, issue a preliminary report b. The specimen is under-decolorized and should be repeated before giving the clinician an interpretation c. The specimen was inappropriately collected, ask the clinician to recollect the specimen d. The Gram stain was over-decolorized and should be repeated before giving the clinician any information e. In preparation of the Gram stain, saffarin was never placed onto the slide |

B. In evaluating a Gram stain, epithelial cells and/or white blood cells are built in controls that will help you
discern that the process was performed appropriately. In a Gram stain, epithelial cells/ WBCʼs should stain pink. If the stain is under-decolorized, as in this case, the epithelial cells are blue. These cells are not as useful in interpreting over-decolorization, as they will be pink in both appropriately decolorized and over-decolorized specimens. If saffarin was not used, there would be no evidence of pink coloration and the epithelial/ WBCʼs would be colorless. |
|
|

While examining the plates from a wound specimen that came from the operating room, you identify tiny, white
creamy colonies that appear to be yeast, mixed with some larger white colonies. You notice that the plates were cultured late the previous evening, but you do not want to delay your identification and susceptibility another day. You decide to carefully isolate only the larger colonies and perform disc diffusion susceptibility testing on a Mueller-Hinton plate. Based on the image, what is the BEST interpretation of this test? a. Based on the growth of small colonies within the zone of inhibition, the organism is susceptible to TE b. Based on the growth of small colonies within the zone of inhibition, the organism is resistant to TE c. The growth of small colonies within the zone of inhibition indicates that there is mixed growth d. The growth of small colonies within the zone of inhibition indicates that the organism has a delayed resistance to TE e. The growth of small colonies within the zone of inhibition indicates that the organism has delayed susceptibility to TE |
C.This picture is an example of mixed growth. A report should not be finalized when mixed growth is seen.
Growth of colonies within the clear zone typically indicates mixed growth, and colonies showing mixed growth should be subcultured, reidentified and retested. Occasionally, this picture can indicate mutant organisms growing in the clear zone, which will eventually become resistant to the antibiotic. For staphylococci and enterococci only, growth within the zone of inhibition around an oxacillin or vancomycin disc is indicative of resistance. |
|
|

A urine specimen from a middle aged female in received in the microbiology laboratory. You notice on the patientʼs
history that her chief complaint is urinary tract infection symptoms with alkaline urine. You examine the blood agar plate and see >100 k/ml of pinpoint smooth whitish-gray colonies growing on the aerobic blood agar plate. There is no growth on the MacConkey plate. You decide to make a Gram stain and notice that as you try to pick a colony from the plate, the colony is very sticky and difficult to sample. While you wait for the Gram stain to dry, you perform a catalase, which is positive. Examination of the Gram stain reveals small slightly curved Gram positive rods. Based on the Gram stain and other findings, what is the MOST LIKELY diagnosis? a. Staphylococcus saprophyticus b. Corynebacterium urealyticum c. Escherichia coli d. Enterococcus fecalis e. Stenotrophomonas maltophilia |
Answer 7a: B.
|
|
|
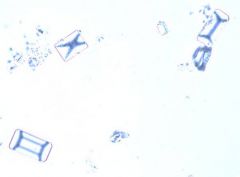
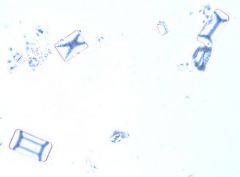
Based on the image and the diagnosis, what type of crystals are commonly found in the urine of these patients?
a. Calcium oxalate b. Tyrosine c. Urate d. Struvite (triple phosphate) e. Cystine |
D. C. urealyticum is one of the more frequently isolated clinically significant Corynebacterium species in
clinical specimens, often responsible for urinary tract infections. Gram stain reveals Gram positive, slightly curved rods. C. urealyticum is catalase positive and strongly urease positive. C. urealyticum urine splitting capability results in alkaline urine and the formation of struvite crystals, which have the easily identifiably “coffin-lid” appearance. Colonies tend to be sticky when sampling from agar and are therefore difficult to remove. Cystine crystals are hexagonal. Tyrosine crystals are needle like. Calcium oxalate crystals are square with a three dimensional point and resemble envelopes. Urate crystals are small, clear, rounded circular objects often with striations radiating from the center. |
|
|
|
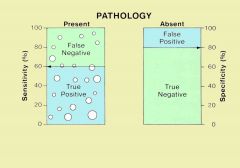
the probability that the test will be negative among patients who do not have the disease
|
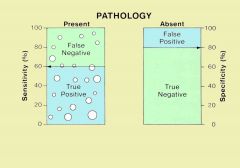
Sp = TN / (TN + FP)
A large specificity means that a positive test can rule in the disease. David Sackett coined the acronym "SpPIn" |
|
|

|
|
|
|

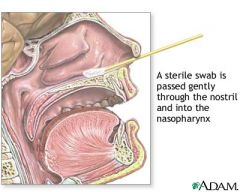
A patient is admitted to the hospital and the clinician orders a nasal swab to screen for methicillin resistant
Staphylococcus aureus (MRSA). The swab is received in the microbiology laboratory and is plated onto a CHROMagar MRSA plate. Based on the growth you see in the image, you perform a latex agglutination test, which is positive. The BEST interpretation of this specimen is: a. The growth indicates that the organism is a methicillin resistant Staphylococcus aureus b. The growth, not the color, indicates that the organism is Staphylococcus aureus and that it is sensitive to methicillin c. The color of the organisms indicate that the organisms growing on the plate are methicillin resistant Staphylococcus aureus d. The color of the organisms indicate that the organisms growing on the plate are methicillin sensitive Staphylococcus aureus e. The color of the organism growing on the plate is suggestive of growth of a red pigmented Serratia species |
Answer: C. CHROMagar MRSA is a qualitative method to detect nasal colonization by methicillin resistant S. aureus.
This test is only a screening test that is performed on anterior nares swab specimens. CHROMagar is a selective and differential medium that incorporates cefoxitin and specific chromogenic substances to detect MRSA. Growth alone does not confirm that the organism is methicillin resistant S. aureus. The mauve-colored colonies confirm methicillin resistant S. aureus. If the organisms are not pink, the growth is not methicillin resistant S. aureus. Organisms other than MRSA can grow and produce a blue or green color, white or no color at all. Coagulase positivity can then be confirmed. Serratia should not grow on this selective media. |
|
|
|
You identify a Klebsiella pneumoniae on a plate from a respiratory specimen. To test the sensitivities for the
organism you use an automated minimum inhibitory concentration (MIC) device. The sensitivity results are ready the next morning and you review the report before sending out the final results. The report shows that the organism is sensitive to all antibiotics. What is your MOST APPROPRIATE next step? a. Finalize the report with the given sensitivities and send the report to the clinician b. Leave the sample on the automated MIC device for another 24 hours to give the machine more time to evaluate the sensitivities c. Finalize the report, stating that the organism is resistant to Ampicillin, despite the MIC results, since you know that all Klebsiella are intrinsically resistant d. Replate, incubate and repeat you initial tests that were used to identify the organism as Klebsiella pneumonia e. Repeat sensitivities with an alternate method, such as Kirby Bauer disc diffusion |
E. Ampicillin is a β-lactam antibiotic, for which Klebsiella species are intrinsically resistant. Klebsiella
organisms are typically sensitive to all other antibiotics. This result is most likely inaccurate, and should not be reported without rechecking the results. Leaving the specimen on the automated MIC device is not effective and will not yield correct results. The best approach for an automated MIC result of a Klebsiella organism that does not show resistance to Ampicillin is to manually check the sensitivity, by a method such as Kirby Bauer disc diffusion. Some labs will also repeat the sensitivities on the automated MIC device. |
|
|
|
All of the following are required to activate Factor X in vivo, except:
Ca++ ATP platelet surface Factor VIIIa Factor IXa |
B. ATP.
The activation of Factor X is central coagulation because active Factor X is responsible for activating thrombin with Factor V as a cofactor. The platelets are involved with coagulation through increased phosphatidyl inositol on their surfaces, thus facilitating factor interaction. |
|
|
|
How does tissue factor pathway inhibitor inhibit coagulation?
inhibition of tissue factor-Factor VIIa-Factor Xa complex conversion of thrombin to prothrombin uncoupling Factor XII-dependent crosslinking of fibrin binding and hiding tissue factor on the endothelial surface consumption of activating ATP |
A. INHIBITION OF TISSUE FACTOR-FACTOR VIIA-FACTOR XA COMPLEX.
TFP1, also know as lipoprotein-associated coagulation inhibitor, anticonvertin, or extrinsic pathway inhibitor, depending who you ask, functions predominantly by inhibiting the critical first step of coagulation, the formation of the tissue factor-Factor VIIa-Factor Xa complex. |
|
|
|
S. bovis
|
associated with colon CA
|
|
|
|
60-80% of all vWD cases; quantitative defect
decreased levels of vWF are detected (10-45% of normal, i.e. 10-45 IU). |
Type 1 vWD
|
|
|
|
20-30%; qualitative defect
normal levels of vWF, but the multimers are structurally abnormal, or subgroups of large or small multimers are absent. Four subtypes exist: 2A, 2B, 2M and 2N. |
Type 2 vWD
|
|
|
|
abnormality of the synthesis or proteolysis of the vWF
small multimer units in circulation. Factor VIII binding is normal. low ristocetin co-factor activity compared to the von Willebrand's antigen. |
Type 2A
|
|
|
|
"gain of function" defect leading to spontaneous binding to platelets and subsequent rapid clearance of the platelets and the large vWF multimers. A mild thrombocytopenia may occur.
The large vWF multimers are absent in the circulation and the factor VIII binding is normal. Like type 2A, the RiCof:vWF antigen assay is low when the patient's platelet-poor plasma is assayed against formalin-fixed, normal donor platelets. However, when the assay is performed with the patient's own platelets ("platelet-rich plasma"), a lower-than-normal amount of ristocetin causes aggregation to occur. This is due to the large vWF multimers remaining bound to the patient's platelets. Patients with this sub-type are unable to use desmopressin as a treatment for bleeding, because it can lead to unwanted platelet aggregation. |
Type 2B
|
|
|
|
This is caused by decreased or absent binding to GPIb on the platelets. Factor VIII binding is normal.
|
Type 2M
|
|
|
|
deficiency of the binding of vWF to factor VIII.
normal vWF antigen level and normal functional test results but has a low factor VIII. some 2N patients may have been misdiagnosed in the past as having hemophilia A, and should be suspected if the patient has the clinical findings of hemophilia A but a pedigree suggesting autosomal, rather than X-linked, inheritance. |
Type 2N (Normandy)
|
|