![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
what are the time parameters for acute vs. chronic abdominal pain? |
acute: less than 3 months chronic: more than 3 months
|
|
|
symptoms of GI |
- abdominal pain - indigestion - n/v - anorexia, early satiety - dysphagia or odynophagia - change in bowel function - diarrhea; constipation - jaundice - PMH - FMH |
|
|
symptoms of urinary & renal |
- suprapubic pain - dysuria, urgency, frequency - hesistancy, decreased stream in men - poly uria or noctuira - urinary incontinence - hematuria - kidney or flank pain - ureteral colic - PMH |
|
|
colorectal cancer screening |
age 50-75 - fecal occult blood testing annually - fecal occult blood testing can lead to dx of colon cancer - screening colonoscopy every 7-10 years - age 76- 85 if never screened than individual - > 85 do not screen, competing causes of mortality preclude mortality benefit that outweighs harm |
|
|
which patients are high risk for colorectal cancer screening? |
- personal hx of colorectal cancer or adenoma - first degree relative with colorectal cancer or adenoma - PMH of breast ovarian or endometrial cancer - PMH of ulcerative colitis or Chron's - FMH of familial adenomatous polyposis; herditary non- polyposis colorectal cancer |
|
|
how do you assess abd pain? |
- take a careful, orderly history - character of the pain: have pt describe in own words - location of pain: have patient point to the pain - radiation of the pain - factors precipitating and relieving abd pain: food - pt assessment of pain severity 0-10 - assess if the pt looks as they are rating the pain - if pt says 8/10 pain, make sure to ask them if they have a high tolerance to pain |
|
|
types of abdominal pain: visceral pain |
- occurs from distention or stretching of organs - difficult to localize - ischemia can stimulate visceral pain fiber - varies in quality - described as gnawing, burning, cramping or aching - severe can be associated with sweating, pallor, n/v |
|
|
types of abdominal pain: parietal pain |
- inflammation in the parietal peritoneum - it is steady, aching pain - more severe than visceral - located over affected structure - worse with movement or coughing - patient prefers to lie still ex: pertitonitis (acute abdomen) |
|
|
referred pain |
pain felt at distance sites which are innervated at approximately the same spinal levels as the disordered structure
- develops as pain intensifies - usually localized |
|
|
differentials by location: RUQ |
- acute cholecystitis, biliary colic - acute hepatitis - perforated duodenal ulcer |
|
|
differentials by location: RLQ |
- appendicitis - SBO - Rental calculi - mesenteric enteritis - female: PID, ectopic pregnancy, ovarian torsion - reference: think of ovaries, ectopic pregancies, mesenteric enteritis --> swollen lymph nodes v. basic explanation |
|
|
differentials by location: LUQ |
- acute pancreatitis - gastric ulcer - gastritis - splenic enlargement |
|
|
LLQ |
- diverticulitis - constipation - bowel obstruction - renal calculi - mesenteritc enteritis - female: PID, ectopic pregnancy, ovarian torsion |
|
|
epigastric |
- peptic ulcer disease - GERD - abdominal aortic aneurysm - pancreatic pain |
|
|
periumbilical |
- gastroenteritis - appendicitis - early bowel obstruction |
|
|
diffuse pain |
- accute pancreatitis - mesenteric thrombosis - gasteroenteritis - dissecting or rupture aneurysm - intestinal obstruction |
|
|
pt presents with nausea, what do you ask? |
define it: unpleasant feeling or sensation that person will vomit
- associated with disorders of stomach and duodenum, esp delyaed gastric emptying - autonomic symptoms- increased perspiration, salivation, skin pallor and vagal discharge that may cause bradycardia and hypotension - does it happen on a full or empty stomach? any mouth watering occur? - does it have any relationship to stooling? - association with food, medicine, stooling pattern, change in diet, duration |
|
|
vomiting |
- associated w/ fever, diarrhea, systemic symptoms? - emesis is? billous? food? fecal? blood? coffee ground? remember a teaspoon of blood mixed in stool looks like a lot more than it is
-association with pain: pain prior to vomiting, concern for an acute abdomen - pain after vomiting, non- surgical emergency ie acute gastroenteritis |
|
|
anorexia |
loss of appetite is a most important but nonspecific symptoms - seen with neoplasm, depression, anorexia nervosa, rental failure, viral hepatits, medications, chronic diseases - is r/t food intolerace (ie lactase deficiency) or reluctance to eat bc of anticipated pain - ask about early satiety, seen with hepatitis - ask about abdominal fullness, gastric outlet obstruction, gastric cancer, anticholinergic meds, diabetic gastroparesis |
|
|
dsyphagia |
- food seems to stick, "not go down right" - sugests motility disorder or structural anomalies, can be cancer or GERD - ask about types of food associated wtih dysphagia - solids that progress to liquids cocnern for esophageal cancer |
|
|
odynophagia |
- pain with swallowing - can be medication induced from aspirin or NSAID - consider esophageal ulcertion |
|
|
bowel function |
- ask about frequency, consistency, color, straining, hx of constipation or diarrhea, changes in bowel function, is it associated with abdominal pain? - if complaining of diarrhea ask about recent travel, foods, medications, exposure to ill contact, systemic symptoms - diarrhea: presence of mucus, occurs at night, greasy or oily, dose the stool float? - blood in stool, melena is an upper GI bleed that presents as black and hematochezia is a lower GI bleed that presents as red
tiny bit of blood? consider hemorrhoids |
|
|
jaundice |
- extrahepatic- biliary obstruction - intrahepatic: viral hepatitis, alcoholic hepatitis, drugs, sepsis, malignancy, sickle cell
|
|
|
risk factors for liver disease r/t jaundice |
- hepatits A: recent travel with poor sanitation - hep B: exposure to infectius bodily fluids - hep C: IV drug use, blood transfusion - alcohol use - meds - gallbladder surgery or disease |
|
|
urinary tract |
- ask about difficulty passing, frequency, dysuria, urgency, nocturia, altered urinary stream, associated pain - hematuria - kidney - trouble with incontinence: ie stress increased abd pressure, increase bladder pressure to exceed urethral sphincter tone, due to poor urethral sphincter tone or poor support of bladder - urge (overactive bladder) urgency is immediately followed by involuntary leaking due to uncontrolled detrusor muscle - overflow: neurologic disorder or obstruction limits emptying until bladder is overdistended - functional; imparied cognition, MSK or mobility |
|
|
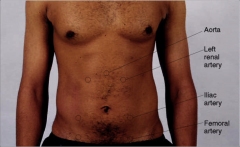
abd physical exam |
- inspect abdomen - auscultate: bowel sounds, arteries - abdominal aorta, renal, iliac, femoral - percuss: abd, liver, spleen - palpate: abd, liver, spleen |
|
|
inspect the abd |
- demeanor - contour - scars and striae - engorged veins - visible peristalsis - visible pulsation - hair distribution - evidence of hernia
|
|
|
how do you get a hernia to pop up? |
ask the pt to bear down |
|
|
what do you think about when you see a pt with abnormal pubic hair? |
- metabolic problem |
|
|
hernias |
- ventral hernias result form defects in the abdominal wall - they are typically classified by etiology and location - result from prior surgery (incisional): muscle gets weak and bowel protrudes - spontaneously, epigastric, umbilical, femoral, inguinal |
|
|
describe an incisional hernia |
- have a bump, hernia can be reducable if it's not reduceable it could be a tumor or mass |
|
|
where are inginal vs femoral hernias? |
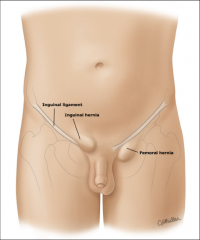
inguinal is above the penis
femoral is to the pt's left of the penis |
|
|
lipoma |
subcutaneous tumors - benign fatty tumors - small or large - soft and lobulated - moveable under the skin |
|
|
how long do you listen to each quadrant to declare no bowel sounds? |
2-5 mins in each quadrent |
|
|
where do you ausculate vascular sounds? |
|
|
|
how do you percuss? |
tympany to dullness |
|
|
what do you hear when you precuss: obesity ascites
|
obesity: tympany with scattered dullness ascites: tympany in the middle with dullness on the sides |
|
|
fluid wave test |
distinguish bt dilated loops of bowel, fat, free fluid abdomen is distended only fluid will transmit a pressure wave
fix midline with hand, hold your hands and tap the other plank
if fluid exists the fluid will touch your opposite hand |
|
|
percussion of liver span |
normal liver spans 4-7 cm in midsternal line 6-12 cm in right midclavicular line
start from typanic until it changes to dullness, usually at or just below the costal margin
start from around the ribs and go down, mark and measure from both sides |
|
|
palpate the spleen |
percuss LL anterior chest wall noting the extent of tympany
tympany is promident then spleen enlargement is unlikely
lowest interspace in left anterior axillary line, if tympany is heard as the patient to take a deep breath
as you percuss in the same place if it's normal, typany will persist which is negative
when spleen is enlarged tympany will turn to dullness |
|
|
light palpation |
looking for tenderness, muscular resistance, guarding - one hand - light gentle motion |
|
|
deep palpation |
looking to identify masses, tenderness, pulsation and any mobility with respiration or pressure from examining hand
- 2 hands - deeper penetrating |
|
|
palpate liver- hook method |

|
|
|
smooth, large liver |
- cirrhosis may produce an enlarged liver with a firm, nontender edge - the liver is not always enlarged in this condition though andmany other diseases may produce similar findings - an enlarged liver with a smooth, tender edge suggests inflammation as in hepatitis or venous congestion, as in right sideed heart failure |
|
|
irregular, large liver |
- an enlarged liver that is firm or hard and has an irregular edge or surface suggests malignancy
- there may be one or more nodules
- the liver may or may not be tnender |
|
|
catching the spleen |
- lie on right side - knee and hip flexed - take a deep inspiration - palpate for splenic edge |
|
|
what do you do/ look for assessing acute abdomen/peritonitis |
- cough test - guarding - rigidity - rebound
|
|
|
cough test |
have pt cough and identify where the pain is located |
|
|
guarding |
- tensing of the abdominal wall muscles to guard inflammed organs within the abdomen from the pain of pressure |
|
|
rigidity |
involuntary reflex contractions of the abd wall that persists over the enitre exam |
|
|
rebound |
deep palpation causes increased pain when pressure with quick release - ask the pt, "which hurts more, when I press in or let go?" if + withdrawal produces pain |
|
|
presentation of acute abdomen |
- patient is lying very still, not moving - pain can be referred to either shoulder - fever - temp - n/v - abdominal distention - generalized inflammation of the peritoneal layer of the abd cavity
|
|
|
what causes an acute abd? |
- appendicitis - cholecystitis - perforated bowel |
|
|
acute appendicitis |
just below the middle of a line joining umbilicus and the anterior superior iliac spine. Right rectal tenderness - inflammation of appendix with distention or obstruction - peri umbilical pain migrating to RLQ pain - pain, mild cramping to severe - n/v/ anorexia may be present - lasts 4-6 hours, can come and go - evaluate for inflammation testing for psoas, obturator, rosving - concern for rupture and acute abdomen |
|
|
psoas test |
+ indicates appendicitis an enlarged appendix may increase RLQ pain
raise right leg against resistance and if the pt has pain then it's +
roll on left side, extend leg and see if there's any pain, if so + |
|
|
obturator test |
sign of appendix irritation obturator lies close to appendix, when it's stretched bc of appendix inflammation
flex pt's leg at the hip and the knee, internally rotate the hip which stretched the internal obturator muscle |
|
|
rovsing sign |
press slowly and gently in the LLQ then quickly release. suddent pain in RLQ is + rovsing sign
|
|
|
cholecystits |
- inflammation of the gallbaldder usually from obstructing the cystic duct of the gallbladder - may have history of biliary colic pain - steady aching pain, RUQ radiating to back or right scapula - Jarring deep breathing increases pain - associated with anorexia, vomiting, fever |
|
|
murphy sign |
+ is indication of gall bladder inflammation or inflammation of liver
hook fingers of your right hand under the costal margin, ask pt to take a deep breath tenderness with a sudden stop in inspirator effort tenderness with a sudden stop in inspiratory effort is a positive sign |
|
|
acute pancreatitis |
- epigastric tenderness, rebound tenderness, abdomen soft - pain radiates to the back - severe, dull, constant - worse when supine, better with sitting or fetal position - associated with n/v - associated with alcohol intake, previous attack, heavy meal - abdominal distention, LUQ and epigastric tenderness - NEGATIVE murphy sign - can be associated with fever, jaundice |
|
|
acute diverticulitis |
usually involves sigmoid colon and resembles left-sided appendicitis
- pain is sudden, severe and often located in the lower left side of the abdomen - change in bowel habits - abdominal tenderness - fever, n/v - bloadting - hx of diverticulosis |
|
|
gastroesophogeal reflux |
- impaired esophageal motility - incompetent esophageal sphincter - h. pylori/ hernia - chest or epigastric pain - burning, gnawing, regurgitation of food - aggravated by bending over, lying down after eating - risk factors: smoking, alcohol, fatty foods - risk for barrets esophagus >> esophageal cancer |
|
|
Peptic ulcer diease |
- gastric or duodenum - H. pylori often present - prolonged NSAID or aspirin use - epigastric pain radiating to back - gnawing, burning, aching, pressing or hunger like pain - gastic (worse with eating) - duodenal- pain wakes at night, intermittent, worse after eating |
|
|
irritable bowel syndrome |
- functional change in frequency or form of bowel movements - symptoms present for at least 12 weeks in preceeding 12 months - does not need to be consecutive - 2 out of three: 1) improves with pooping 2) onset with change in stool frequency 3) onset with change in stool form
- pain usually crampy, lower abs distention, flatulence, nausea - abnromal stooling: > 3 BM/day < 3 BM/ week - unknown etiology - young and middle aged adults, esp women |
|
|
what are two diseases within inflammatory bowel disease? |
1) ulcerative colitis 2) chron's disease |
|
|
ulcerative colitis |
- inflammation of the mucosa and submucosa of the rectum and colon with ulceration - usually extends proximally from the rectum - stools are soft, watery with blood - typically reccurent, presistent, diarrhea may awaken at night - mild cramping, lower generalized abdominal pain - anorexia, weakness - young people - increased risk of colon cancer |
|
|
chron's diease |
- chronic, transmural inflammation of the bowel wall - mouth to anus, skip pattern - small, soft loose to watery stool, usually free of blood - crampy, periumbilical or RLQ or diffuse pain - anorexia, low fever, weight loss - late teens - increased risk of colon cancer |