![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
138 Cards in this Set
- Front
- Back
|
EZ93 What is the chemical used in sodalime to indicate exhaustion? |
ANSWER A
Components of Sodalime NaOH 5% Ca(OH)2 94% Water Ethyl violet as indicator Binders |
|
|
2. Repeat- Main heat loss in anaesthetic for neonate
A. vasodilatation B. radiation C. convection D. conduction E. evaporative |
ANSWER B
|
|
|
The most appropriate method for improving oxygenation during one lung anaesthesia, after institution of an FiO2 of 1.0, is application of |
ANSWER A |
|
|
4. Child with murmur- what would make it more likely for you to investigate if you heard the murmur |
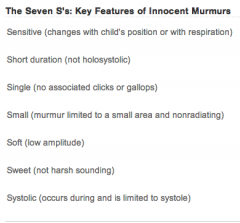
EXCLUDE ON HISTORY |
|
|
5. Repeat- Single lumen intubation after multiple attempts of difficult intubation, you put in a bronchoscope after and the tip is in the trachea. The structure B you seen corresponding to?
|
Trachealis is posterior, use this to orientate |
|
|
7. Repeat- Neonate to drug addicts found by grandmother in the house, brought into ed, mildly jaundice, slight tachycapnic. ABG PH 7.54, PaCO2 46, pO2 74, HCO 13 |
ANSWER B |
|
|
ET03 [Repeat] Jehovah's witness refused blood- you have told him you refuse to do the surgery/anaesthesia for his own good. Ethical principle: |
ANSWER A |
|
|
9. Patient with aortic stenosis, the signs indicate poor prognosis |
Signs of severity 7. Presence of Thrill |
|
|
Which is the best predictor of poor prognosis with aortic stenosis? |
ANSWER B |
|
|
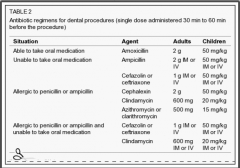
10. New- Patient indicated for prophylaxis of infective endocardititis |
ANSWER D |
|
|
11. Circuit disconnection during spontaneous breathing anaesthesia |
ANSWER D |
|
|
12. Which is NOT a disadvantage of drawover vaporiser versus plenum vaporiser?
|
ANSWER C
Disadvantages |
|
|
PZ130 Which drugs below does not need dose adjustment in renal failure patient |
ANSWER A
|
|
|
14. Repeat- Child after gas induction, LMA insertion without IV cannula- desaturate to 90%. Next step of action? |
ANSWER B
Remove cause (sputum/LMA/blood etc) Apply CPAP Deepen Anaesthesia (volatile/propofol) Consider Sux (iv/im/intralingual) |
|
|
PZ128 Patient on cisapride. What drug NOT to give in recovery? |
ANSWER A |
|
|
16. Repeat- Which herbal supplement reacts with tramadol?
A. Ephedra B. St John's wort |
ANSWER B |
|
|
17. Fat: blood coefficient: A. N2O < D < S ~ I |
N2O 2.3 |
|
|
18. Immunology mediated heparin induced thrombocytopenia
A. Intravascular thrombosis |
HITTS |
|
|
19. Repeat- Half life or tirofiban? |
A |
|
|
TMP-131 Repeat- Troponin can be detected for how long: |
A
|
|
|
21. Neonate intubation distance at lips |
Neonate: - Weight + 6 Infant: - Age/2 + 12 (at lips) - Age/2 + 15 (at nares) |
|
|
22. New - 72 year old has had hip replacement surgery and 3 days postop has a pulmonary embolus. He is fully heparinised, but still dyspnoeic, clammy, BP 80/40, pulse 120 and CVP 18. The most appropriate next step is |
ANSWER B |
|
|
23. Repeat- The test to diagnose pulmonary embolism
A. CT pulmonary angiogram B. Echocardiogram C. Electrocardiogram D. Ventilation-perfusion scan |
ANSWER A
|
|
|
24. Repeat- Finding on haemophilia A patient
A. Female haemarthrosis B. Male haemarthrosis C. Normal PT, abnormal APTT D. Abnormal PT, normal APTT |
ANSWER C |
|
|
25. New- LSCS for foetal distress, meconium stained liquor. Management of baby |
ANSWER D
If vigorous - routine antenatal care If floppy - post partum tracheal suctioning |
|
|
26. Repeat- 36yo male with sickle cell anaemia Hct 0.3 with close foot fracture, what is true |
ANSWER B |
|
|
27. New- An elderly lady has a closed neck of femur fracture and presents to ED. She is in chronic AF and on warfarin. INR is 2.6 and she is not bleeding. It is 9am and she is scheduled for repair the following day. According to current guidelines, how should her warfarin be reversed? |
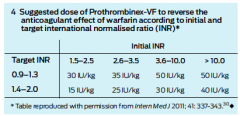
ANSWER
Vit K 3mg iv + recheck INR mane
Given Prothrombinex as per Box 4
If Bleeding, consider Vit K + FFP dependent on INR |
|
|
28. Repeat- Marfan syndrome. All EXCEPT- |
Cardiac Manifestations |
|
|
29. New- Subarachnoid haemorrhage patient. What percentage rebleed in the first 24hours
A. <5% B. 5-10% C. 10-15% D. 15-20% E. >20% |
ANSWER A |
|
|
30.TMP11B30 New- Post delivery neonate did not breath post stimulation by midwife, not vigorous, heart rate drop from 140 to 90bpm. Next step of action |
ANSWER B |
|
|
31. New- The safe maximal pressure for endotracheal cuff at the lateral side of the trachea |
ANSWER C |
|
|
32. Repeat- Allergy to penicillin- cross reaction to neuromuscular blocker
|
?
|
|
|
33. New- Patient with mastocytosis. Intraop would probably be:
A. Severe hypotension |
A
|
|
|
34. Repeat- Complication of celiac plexus block
A. Hypertension B. Failure of erection C. Constipation D. Paraplegia E. L3,4 lumbar pain |
ANSWER D
Complications • Severe hypotension may result, even after unilateral block. • Local pain during procedure • Diarrhoea • Intramuscular injection into the psoas muscle. • Bleeding due to aorta or inferior vena cava injury by the needle. • Intravascular injection (should be prevented by checking the needle position with radio-opaque dye). • Upper abdominal organ puncture with abscess/cyst formation. • Paraplegia from injecting phenol into the arteries that supply the spinal cord (prevented by checking the needle position with radio-opaque dye). • Lumbar nerve root irritation (injected solution tracks backwards towards the lumbar plexus). • Sexual dysfunction (injected solution spreads to the sympathetic chain bilaterally) = inability to ejaculate • Pneumothorax • Shoulder/chest/pleuritic pain/hiccupping – diaphragmatic irritation • Haematuria from renal pouncture |
|
|
35. New- Post epidural and LSCS, the next day patient have persistent paraesthesia anterior thigh. What other injuries would indicate more of nerve roots instead of peripheral nerve injuries |
ANSWER A
Hip Flexion/Thigh Adduction - Femoral + Obturator (i.e. L1-L4) Knee Flexion/Plantar Flexion - Sciatic Urinary Incontinence - pudendal nerves Foot Drop - Common Peroneal |
|
|
36. Repeat- Nerve supply to the upper eyelid- |
Sympathetic from Superior Collicus ganglion and oculomotor nerve. |
|
|
37. LUSCS for failure to progress. Spinal is inserted uneventfully. Next day the patient has foot drop. The most likely cause is? |
ANSWER D |
|
|
38. You are asked to see a 60 y.o. male 2 days following a cervical laminectomy because he has new new neurological symptoms in his right arm. The surgical team think these may be due to poor patient positioning. The sign that would most help differentiate C8-T1 nerve root injury from an ulnar nerve injury is |
ANSWER D |
|
|
39. ECG- which does NOT have abnormal Q waves: |
ANSWER A |
|
|
40 The QT interval may be prolonged by each of the following EXCEPT |

ANSWER C |
|
|
41. Post CEA on ward, patient seizes. BP has been hard to control. What to do to prevent further seizures? |
ANSWER A |
|
|
42. Repeat- Post local anaesthetic block in difficult intubate patient- patient seizure. What would you give? |
ANSWER A
|
|
|
43. Patient presents with carcinoid syndrome and developes hypotension intraoperatively. Best drug to treat it is: |
ANSWER D |
|
|
44. Repeat- Allergic question, which is true |
ANSWER D |
|
|
45. AB50 ANZCA version [2005-Sep] Q120 |
ANSWER A |
|
|
46. New- After transfusion of 5 unit of FFP what is least likely to occur |
ANSWER D |
|
|
47. Severe asthmatic- tachycapnia, HR120, speaking in words, pH 7.45, pCO2 46, pO2 96, HCO3 24. Then given nebulised salbutamol continuously, nebulised ipratropium bromide, and hydrocortisone- The next step: |
ANSWER Magnesium
|
|
|
48. AC62b ANZCA version [2003-Apr] Q144, [2004-Apr] Q98, [2004-Aug] Q44, [Jul06] Q23 |
ANSWER B
|
|
|
49. New- There is evidence to avoid BIS <40 for more than 5 minutes because |
ANSWER C |
|
|
50. New- Most common cause of paediatric post anaesthesia cardiac arrest |
ANSWER B |
|
|
51. New- Post cervical spine op, there is bulging noted under the incision site. Patient desaturated, combative, keep pulling off the oxygen facemask. Next course of action |
ANSWER A
RSI most practicable, however may lead to difficult airway.
Inhalational induction safer if can restrain patient. |
|
|
52. New- What drug known to cause prolong QT and risk of Torsades de Pointes |
ANSWER B |
|
|
53. New- During cardiac catheterisation (?) patient become BP 80/60, HR 110, CVP 16. What is the next most important investigation |
ANSWER A |
|
|
54. Intraop hyperfibrinolysis- how to diagnose (euglobulin lysis time NOT an option in the answer) |
ANSWER A
|
|
|
55. New- 75yo patient seen for femoral bypass surgery, no significant cardiac risk factor. He will be admitted 3 days prior to operation. You decided NOT to start on beta blocker and you are justified because: |
ANSWER A |
|
|
56. New- You see a man in his 60s in clinic 1 week prior to laparoscopic cholecystectomy. He has dilated cardiomyopathy with an ejection fraction of 30%, but does not get dyspnoeic with normal activities of daily living. What is the most appropriate management of his heart failure? |
ANSWER C |
|
|
57.EZ80 Repeat- A line isolation monitor protects against microshock |
ANSWER C |
|
|
58. AT27 [Apr07] Q108 |
ANSWER E
|
|
|
59.RB53 Repeat- Post dural punture headache |
ANSWER D |
|
|
60. New- Patient ingested 500mg/kg aspirin. In ICU, the most effective method to remove aspirin |
ANSWER B
|
|
|
61. Repeat- The most effective method of decrease renal impairment in AAA surgery
|
ANSWER E
Maintain renal flow |
|
|
62. |
ANSWER C |
|
|
63. Repeat- The most effective method for cerebral protection in aortic arch aneurysm repair |
ANSWER B
Maintains cerebral perfusion, can be combined with DHCA |
|
|
SF53 ANZCA version [2001-Apr] Q6, [2001-Aug] Q4, [2003-Aug] Q66, [2004-Apr] Q55, [Mar 10],[Aug10] |
ANSWER C |
|
|
65. Repeat- Most common signs of malignant hyperthermia- |
ANSWER A |
|
|
66. New- The below would increase A-a oxygen gradient Except |
ANSWER B |
|
|
TMP-104 [Mar10] [Aug10] |
ANSWER A
|
|
|
68. Repeat- Patient cough during interscalene block- insertion needle should be directed- |
ANSWER posterior |
|
|
69. New- Interscalene block after injection of 2ml bupivacaine- patient seizure. Most likely injected to |
ANSWER B
|
|
|
70. New- Post intubation, you manual ventilate and noted patient high airway pressure. What would you do next |
ANSWER B
|
|
|
71 |
ANSWER B
|
|
|
72. New- Modified Cormack and Lehane grade - You cannot see beyond the epiglottis and there is a little space between the epiglottis and the posterior pharyngeal wall (? remembered as epiglottis touching posterior pharyngeal wall) |
ANSWER D
Grade I: Complete glottis visible. |
|
|
73Stellate ganglion block associated with all except: |
ANSWER C |
|
|
74. Repeat- Most safe side to insert subtenon block |
ANSWER A
|
|
|
75. Compared to retrobulbar block, peribulbar block is associated with |
ANSWER D
|
|
|
76. Repeat- Diastolic dysfunction Not caused by |
ANSWER A |
|
|
ANZCA Version [Apr07] |
ANSWER C |
|
|
78. Lumbarsacral nerve does not supply: |
ANSWER A |
|
|
79. Repeat- Relative humidity of fully saturated air at 20degree and 37 degrees- |
Absolute humidity |
|
|
80.IC90 Repeat- Trauma patient best indicator of good resuscitation (?)- |
ANSWER A
|
|
|
81. New- Pregnant patient seatbelt, driver- involved in car accident. Suddenly developed severe central chest pain, HR 110, BP 154/80, RR 26, Sat 100%. The most likely cause? |
ANSWER A
|
|
|
82. New- ASD murmur heard at |
ANSWER C
|
|
|
84. TMP-Jul10-038 |
ANSWER D |
|
|
83. AB58 ANZCA version [Jul07] Q141 |
ANSWER D
Elimination half life 2.4-4-4 hrs |
|
|
85 TMP-Jul10-044 |
ANSWER E
|
|
|
86. TMP-Jul10-045 How quickly does the CO2 rise in the apnoeic patient ? |
ANSWER C
From Miller, 1st minute Co2 increases by 6 mm Hg all subsequent minutes 3 -4 mm Hg |
|
|
87. New- Apnoeic oxygenation in obese patient can be increased by |
ANSWER E |
|
|
88
A. Flaccidity of the leg muscles |
ANSWER A |
|
|
89 TMP-Jul10-048 |
ANSWER A
first severe pulmonary vasoconstriction ,Rt ventricular failure ,then Lt ventricular failure and pulmonary oedema ,embolism is probably a misleading name,its actual pathology is anaphylaxis to foetal tissues |
|
|
90. New- Post partum sudden collapse, suspected amniotic fluid embolism. The consistent finding is: |
ANSWER E
|
|
|
91 TMP-Jul10-049 |
ANSWER A
|
|
|
92. RH12b [Mar92] |
ANSWER A
|
|
|
93. TMP-Jul10-054 |
ANSWER A
Incidence measures the rate of occurrence of new cases of a disease or condition. Prevalence measures how much of some disease or condition there is in a population at a particular point in time. |
|
|
ST19 ANZCA version [2002-Mar] Q62, [2002-Aug] Q59, [2005-Apr] Q58, [2005-Sep] Q50
From this we can conclude that |
ANSWER B |
|
|
95 TMP-121 [Apr08] [Aug08] |
ANSWER C |
|
|
96. TMP-Jul10-062 [Aug10] |
ANSWER D |
|
|
97 |
ANSWER A
|
|
|
98. Which patients do not get pulmonary hypertension
a. ASD |
ANSWER C |
|
|
99 MC157 [Mar10] [Aug10] |
ANSWER B |
|
|
100 |
ANSWER A |
|
|
101. New- Young pregnant patient with moderate mitral stenosis, normal LV function. The best delivery method
A. Epidural anaesthesia LSCS B. Spinal with LSCS C. Epidural analgesia and normal vaginal delivery D. GA LSCS E. Normal vaginal delivery with remifentanil PCA |
ANSWER C
MS is a fixed output valvular disease -transmitral gradient is proportional to CO squared, therefore increasing CO by 50%, will increase the gradient 2.3 fold -generally pregnancy will increase NYHA class by One Aims are to keep the patient at they are -maintain preload -normal HR -maintain afterload MS should be evaluated before pregnancy -prophylactic percutaneous mitral balloon valvotomy -NHYA 2-4 or high PTH high risk of complications and death Treat antenatal with diuretic and beta blockers -care should be taken to avoid hypovolaemia -ACEI are contraindicated in pregnancy Labour and post partum are the most dangerous times -Epidural to blunt sympathetic response (attenuate HR, CO, therefore minimised increasing transmitral gradient) -Most delivery, sudden increase in preload with autotransfusion can lead to APO -Cautious use of Syntocinon during 3rd stage. Vasodilation can cause hypotension with compensatory tachycardia leading to overdistention of LA (due to MS) and AF => APO -AF should be electrically cardioverted. |
|
|
102
PP84b ANZCA version [2005-Sep] Q141 Tracheo-oesophageal Fistula (TOF) A. is associated with cardiac anomalies in approximately 60% of cases B. is associated with oesophageal atresia in approximately 20% of cases C. is more common in males than females D. is usually left sided E. does not usually require contrast studies for diagnosis |
ANSWER E
A. Cardiac in 20% B. Atresia in 80-90% C. 1:1 D. right |
|
|
103
MC30b ANZCA version [2004-Aug] Q128, [2005-Apr] Q55 A patient with pulmonary hypertension secondary to lung disease presents for a laparotomy. Regarding this patient's anaesthetic management A. an alpha-agonist is the inotrope of choice B. hypothermia is protective against rises in pulmonary artery pressure C. isoflurane will tend to decrease pulmonary artery pressure D. ketamine is an appropriate anaesthetic agent E. right heart failure is not a concern |
A patient with pulmonary hypertension secondary to lung disease presents for a laparotomy. Regarding this patient's anaesthetic management
* A. an alpha-agonist is the inotrope of choice - probably true and best answer: o there are No α-1 adrenergic receptors are present in the pulmonary circulation (Blaise, Anaesthesiology, 2003, 99(6):1421) so α-1 agonists are fine and may assist RV function by increasing coronary perfusion pressure (although some prefer dobutamine initially becuase it increases contractility and may pulmonary vasodilate) o the wording is confusing and might subequently change now. Both the Blaise article and Stoelting 5th ed. suggest that causes of hypotension are multifactorial and should be treated accordingly. Specifically pulm HTN crisis requiring inotropy, the 'inotrope' of choice might be milrione (or possibly dobutamine), however R heart ischaemia and low SVR (with fixed PVR) are important causes of hypotension specifically treated with noradrenaline * B. hypothermia is protective against rises in pulmonary artery pressure - false o Hypothermia increases PVR (A & A ,Volume 96(6), June 2003, pp 1603-1616) * C. isoflurane will tend to decrease pulmonary artery pressure - false o PVR does not change with volatiles except N2O which does increase PVR (Stoelting Pharmacology p47) o Isoflurane has no effect on baseline pulmonary vessel tone. (Blaise, Anaesthesiology, 2003, 99(6):1421) * D. ketamine is an appropriate anaesthetic agent - false o 'In patients who have pulmonary artery pressure, ketamine seems to cause a more pronounced increase in pulmonary than systemic vascular resistance' (Miller, p348) o 'The sympathomimetic properties of ketamine may preclude use in the setting of pulmonary hypertension (Yao, p96) o In-vitro ketamine increases PVR in rat lung...(and)...ketamine attenuates endothelium-dependent pulmonary vasorelaxation in response to acetylcholine and bradykinin ...(and)...sympathetic innervation of the pulmonary circulation does exist (Blaise, Anaesthesiology, 2003, 99(6):1421) * E. right heart failure is not a concern - false |
|
|
104. New- Neonate desaturate faster than adult at induction because
A. FRC decrease more B. Faster onset of induction agents C. More difficult to pre-oxygenation |
???
Reasons for neonatal desat 1. High metabolic rate 2-3 x adult (required mainly for temperature control, high BSA to mass) 2. Small absolute FRC (same as adult 30ml/kg) therefore less oxygen 3. CC >FRC, neonate generates autoPEEP by partial closure of glottis, this is lost at induction, causing airway closure and V/Q mismatch |
|
|
105. New- The cause of hypoxia in one lung ventilation
A. Blood flow through non ventilated lung B. Impairment of hypoxic pulmonary vasoconstriction C. Ventilation perfusion mismatched (?) |
ANSWER A
|
|
|
106. New- Suxamethonium dosage higher in neonates compare to adult because
A. Increased volume of distribution B. Increased pseudocholinesterase activity C. More receptors D. Higher cardiac output (?) E. Decreased sensitivity of nicotinic ACH receptors to suxamethonium F. Faster diffusion away from neuromuscular junction |
ANSWER A
|
|
|
107 TMP-107 [Mar10] [Aug10]
Baby with Tracheo-oesophageal fistula found by bubbling saliva and nasogastric tube coiling on Xray. BEST immediate management? A. Bag and mask ventilate B. Intubate and ventilate C. position head up, insert suction catheter in oesophagus (or to stomach?) D. Place prone, head down to allow contents to drain E. Insert gastrostomy |
ANSWER C
|
|
|
108 NV42 [Apr07] [Jul07]
What do C6/7 motor function do A. flex/extension of fingers B. flex /extend wrist C. shoulder ext rotation / abduction D. elbow pronation/supination E. flexion at elbow |
ANSWER B
|
|
|
109
SF89 [Mar10] Most likely change on CTG with anaesthesia for non-obstetric surgery at 32 wks: A. Loss of beat to beat variability B. No change C. Late decelerations D. Variable decelerationss E. Uterine contractions |
ANSWER A
# Normal CTG under GA = Loss of beat to beat variability, no decelerations. # Normal CTG under neuraxial block without sedation = No change |
|
|
110. New- Indicates autonomic neuropathy except
A. Sinus arrthymias B. Gastric reflux C. Postural hypotension |
ANSWER A
|
|
|
111. Repeat- Best indicator of return function of laryngeal muscle
A. Sustained head lift 5 sec B. Sustained leg lift 5 sec C. TOF 0.9 D. DBS no fade E. Tetanus 50Hz |
ANSWER D
|
|
|
112 MC59b ANZCA version [2003-Apr] Q125, [2003-Aug] Q85, [2005-Sep] Q69, [Mar06] Q48 [Mar10] [Aug10]
In the management of torsades de pointes (polymorphic ventricular tachycardia), all the following drugs may be useful EXCEPT A. amiodarone B. isoprenaline C. [[lignocaine] D. magnesium E. phenytoin |
ANSWER A
|
|
|
113. New- A nulliparous woman in labour for 8 hours with epidural analgesia has a fever 37.6 degrees. The most likely reason for this is
A. altered thermoregulation B. chorioamnionitis C. urinary tract infection D. inflammatory response E. neuraxial infection |
ANSWER D
Epidural associated fever is common, ranging from mild hyperthermia to overt fever. Risk Factors 1. Nullparious 2. Prolonged labor 3. PROM Mechanisms postulated 1. Inflammation: most accepted explanation, unknown if it is infectious or non infectious (women with fever and epidural do not have evidence of chorioamonitis on histology) 2. Altered thermoregulation: hyperventilation during labor is diminished, resulting in reduced heat loss. 3. Effect of opioids: opioids suppress IL-2 formation www.anesthesia-analgesia.org/content/111/6/1467.full.pdf |
|
|
114 Can01-113 What nerve supplies sensation to the larynx above the vocal cords:
A. internal branch of superior laryngeal nerve B. external branch of superior laryngeal nerve C. recurrent laryngeal nerve D. glossopharyngeal nerve E. palatotonsillar nerve |
ANSWER B
|
|
|
115
NN05 ANZCA version [2004-Aug] Q17, [2005-Apr] Q63, [Apr07] (Similar question reported in [1985] [Aug96] [Jul97] [Jul98]) The carotid sinus derives its nerve supply from the A. vagus nerve B. glossopharyngeal nerve C. ansa cervicalis (hypoglossi) D. middle cervical ganglion E. stellate ganglion |
ANSWER B
|
|
|
116. ? Post op pneumonectomy short of breath- investigation
|
??
|
|
|
AC155 [Apr07]
A patient with severe COPD on home oxygen is having an excision of a submandibular tumour under local anaesthesia. The best way to prevent fire in the operating room is: A. seal the surgical site from the patients airway with adhesive drapes B. use bipolar instead of monopolar diathermy C. decr FIO2 to maintain sats 97% D. use alcoholic chlorhex instead of iodine E. add nitrous oxide to the inhaled gases to reduce the FiO2 and provide sedation |
ANSWER B
* A. seal the surgical site from the patients airway with adhesive drapes - potentially correct: "Oxygen is heavier than air, and can therefore accumulate under surgical drapes. This accumulation may be reduced by the use of ‘incise drapes’ that protect the wound from high oxygen concentrations and by tenting surgical drapes to dilute oxygen with room air." (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) The answer will depend on what the examiners mean by adhesive drapes * B. use bipolar instead of monopolar diathermy - definitely correct: "The cutting mode of diathermy is more likely to ignite fuels than the coagulation mode, and fires are more likely with monopolar diathermy than bipolar" (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) * C. decr FIO2 to maintain sats 97% - almost certainly incorrect: "Strategies to reduce the risks posed by high oxygen concentrations include (the) judicious use of oxygen (using the lowest oxygen concentration that provides acceptable haemoglobin oxygen saturations" (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) The key here is acceptable haemoglobin oxygen saturations. "Long term continuous oxygen therapy should be considered for patients with stable chronic lung disease, particularly COPD, who have an arterial PO2 (PaO2) consistently less than or equal to 55 mm Hg when breathing air, at rest and awake. ...Flow rate should be set to maintain PaO2 > 60mmHg (8 kPa) (oxygen saturation level, measured by pulse oximetry [SpO2]> 90%) during waking rest." (McDonald et al, Adult domiciliary oxygen therapy. Position statement of the Thoracic Society of Australia and New Zealand, MJA 2005; 182: 621–626) Note that PO2=55mmHg is equivalent to SaO2 88% * D. use alcoholic chlorhex instead of iodine - definitely incorrect: "Alcohol-based antibacterial skin preparations are one of the more common causes of surgical fires since the withdrawal of flammable anaesthetic agents. They can pool on the body surface (especially umbilicus and suprasternal notch), be wicked into surgical drapes and produce flammable vapours that can accumulate beneath the drapes." (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) * E. add nitrous oxide to the inhaled gases to reduce the FiO2 and provide sedation - definitely incorrect: "Nitrous oxide also supports combustion and is broken down to produce oxygen, nitrogen and heat." (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) |
|
|
118 MN38 ANZCA version [2004-Apr] Q124, [2005-Apr] Q100, [2005-Sep] Q94, [Jul07] [Apr08] [Aug08] [Aug09][Mar10] [Aug10]
Respiratory function in quadriplegics is improved by A. abdominal distension B. an increase in chest wall spasticity C. interscalene nerve block D. the upright position E. unilateral compliance reduction |
ANSWER B
|
|
|
119.92.Pulsus paradoxus is: (the Q was something like - severe asthmatic - when take BP you would find)
A. Reduced BP on inspiration unlike normal (ie normally increased on insp) B. Reduced BP on inspiration exaggerated from normal C. Reduced BP on expiration unlike normal D. Reduced BP on expiration exaggerated from normal E. ? |
ANSWER D
|
|
|
120. New- Pre eclamptic patient post LSCS continue on Mg infusion in ICU. Found to be in respiratory depressed. Next management
A. Calcium gluconate B. IV fluid C. Frusemide |
ANSWER C
From RWH Request magnesium level and review management if: * respiratory rate < 12 breaths/minute * urine output < 100mLs in 4 hours * loss of patellar reflexes * further seizures occur. Response to magnesium toxicity The following clinical signs of magnesium toxicity must be reviewed by a consultant obstetrician/anaesthetist: * urine output <100mL in 4 hours * absent patellar reflexes * respiratory depression. The antidote for magnesium toxicity is: calcium gluconate (10mL of 10% solution over 10 minutes) by slow intravenous injection. The patient requires ECG monitoring during and after administration because of the potential for cardiac arrhythmias. Resuscitation and ventilator support should be available during and after dose administration of both magnesium sulphate and calcium gluconate. |
|
|
121. New- Periop clinic reviewing a patient with chronic/ end stage renal failure. Her calcium found to be low. He most certainly have
A. Primary hyperparathyroidism B. Secondary hyperparathyroidism C. Tertiary hyperparathyroidism |
ANSWER B
Primary hyperparathyroidism causes hypercalcemia (elevated blood calcium levels) through the excessive secretion of parathyroid hormone (PTH), usually by an adenoma (benign tumors) of the parathyroid glands. Secondary hyperparathyroidism refers to the excessive secretion of parathyroid hormone (PTH) by the parathyroid glands in response to hypocalcemia (low blood calcium levels) and associated hypertrophy of the glands. Tertiary hyperparathyroidism is a state of excessive secretion of parathyroid hormone (PTH) after a long period of secondary hyperparathyroidism and resulting hypercalcemia. It reflects development of autonomous (unregulated) parathyroid function following a period of persistent parathyroid stimulation. |
|
|
122. Repeat- How to estimate weight in child-
|
(Age+4) x2
Age |
|
|
123 SG59 [Apr07]
Blunt liver trauma can be treated non surgically if A. No peritoneal signs B. Low Grade injury on CT scan C. Severe COPD D. Haemodynamically stable E. US confirms <500mls peritoneal fluid collection (i thought this was a paracentesis result) |
ANSWER D
|
|
|
124 AZ (Q120 Aug 2008) Preoperative assessment shows a malampati (ML) score of III and thyromental distance (TMD) of < 6cm. A grade 3 to 4 on Cormark and Lehanes is predicted. Compared to the ML score, the TMD is:
A less sensitive, less specific B less sensitive, more specific C more sensitive, less specific D more sensitive, more specific E equal sensitivity an specificity |
ANSWER B
|
|
|
125. New- Compare to Myasthenia gravis, which symptoms is more likely to be Eaton Lambert syndrome?
|
EATON LAMBERT SYNDROME
Myasthenic syndrome Definition: autoimmune NM disorder characterized by IgG Ab to pre-synaptic Ca channels and decreased ACh release • Associated with malignancy 50-60% • Small cell lung Ca CLINICAL • Proximal muscles weakness, esp lower limbs • Strength improves with activity • Although 30% demonstrate fatigability • Myalgia • Tendon reflex is absent • Ocular/bulbar dysfunction • Autonomic dysfunction ANAESTHETIC IMPLICATIONS • Sensitive to both sux and NDMR TREATMENT • Not reverse by anticholinestases • Immunosuppression with steroid • Plasma exchange |
|
|
126 AM41 ANZCA version [2004-Aug] Q15, [Mar06] Q11, [Jul07]
The most frequently reported clinical sign in malignant hyperpyrexia is A. arrhythmia B. cyanosis C. sweating D. tachycardia E. rigidity |
ANSWER D
|
|
|
127 RH26b ANZCA version [2004-Apr] Q126, [Jul07]
To achieve maximum anaesthesia with minimal risk of trauma to veins, the tip of a needle used for a medial peribulbar injection should be advanced no further past the equator of the globe than A. 5 mm B. 10 mm C. 15 mm D. 20 mm E. 25 mm |
ANSWER B
10mm past equator as CEACCP says should not go past posterior border of globe. |
|
|
128 PR04 ANZCA version [1985] [Mar95] [Apr97] [Jul97] [Apr98] [Jul98] [2002-Aug] Q11, [2003-Apr] Q39, [2005-Sep] Q46, [Mar06] Q25
The percentage of the population which is heterozygous as regards pseudocholinesterase, thus having a dibucaine number between 30 and 80, is A. 0.04% B. 0.4% C. 4.0% D. 14.0% E. 40.0% |
ANSWER C
|
|
|
129 ST22 ANZCA version [2002-Aug] Q81, [2004-Apr] Q88, [2004-Aug] Q78
Recognised weaknesses of systematic reviews include all of the following EXCEPT A. publication bias B. duplicate publication C. study heterogeneity D. inclusion of outdated studies E. systematic review author bias |
ANSWER E
|
|
|
130 AA22 ANZCA version [2005-Apr] Q106
The commonest initial presenting feature in anaphylaxis is A. coughing B. desaturation C. hypotension D. rash E. wheeze |
ANSER C
|
|
|
131. New - When stimulating the ulnar nerve with a nerve stimulator, which muscle do you see twitch?
A. opponens abducens B. abductor pollicis brevis C. adductor pollicis brevis D. extensor pollicis E. flexor pollicis brevis |
ANSWER C
Ulnar nerve supplies the intrinsic muscles of the hand, except LOAF |
|
|
132. New - When intubating over a bougie / awake fibreoptic, which direction do you rotate the tube to stop it catching on structures in the glottis
A. no change from normal B. 90 degrees clockwise C. 90 degrees counterclockwise D. 180 degrees E. try either direction |
ANSWER C
|
|
|
133. New - Advantages of off-pump CABG over on-pump CABG
A. decreased transfusion rate B. decreased mortality C. decreased cost D. increased graft patency E. less cognitive impairment F. less stroke |
ANSWER A
CEACCP Hett 2006 Benefits of OPCABG -mortality reduced from 2.9% -> 2.3% and complication rate 12% -> 8% (conflicting results from other studies) -Most studies have shown a reduction in the need for transfusion and other blood products (effect of extracorporeal circulation and hypothermia) -Incidence of stroke is less (no manipulation of aorta resulting in macro and micro embolii) -reduced rise in inflammatory markers No difference -mortality and morbidity is unchange -incidence of AF is similar -short term patency rate are comparable. There is no info on long term patency -no difference in neurological dysfunction |
|
|
134. New - After coronary artery bypass graft surgery, the FRC is
A. increased 40% B. increased 20% C. unchanged D. decreased 20% E. decreased 40% |
ANSWER D
Compared to preop -open sternotomy 55% increase -closure decrease 10% -day 1 decrease 20% |
|
|
135. New - A 60 year old man 24 hours post CABG is confused, oliguric, with BP 80/40, pulse 120. The most appropriate and useful investigation is
A. electrocardiogram B. echocardiogram C. chest x-ray D. arterial blood gas E. coronary angiogram |
ANSWER B
|
|
|
136. Iron deficiency
A. decreased serum ferritin, increased serum iron B. decreased serum ferritin, absence of bone marrow iron C. decreased serum ferritin, normal serum iron D. increased serum ferritin, decreased serum iron E. increased serum ferritin, decreased total iron binding capacity |
ANSWER B
|
|
|
137. New - Why should NSAIDs be avoided in pregnant women >30 weeks gestation?
A. cause neonatal acute renal failure B. increased antepartum haemorrhage C. increased rate of pre-eclampsia D. cause closure of the fetal ductus arteriosus E. increase preterm labour |
ANSWER D
|
|
|
138. A 62 year old man has chronic renal failure. You notice his total serum calcium is 2.05 mmol/L. This is because he has
A. high serum vitamin D B. hypoparathyroidism C. primary hyperparathyroidism D. secondary hyperparathyroidism E. tertiary hyperparathyroidism |
ANSWER D
|