Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
ANDROGENS
|
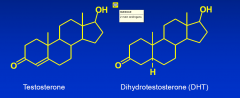
A major class of steroid hormones that develop and
maintain physiological masculine characteristics mainly via binding to the androgen receptor |
|
|
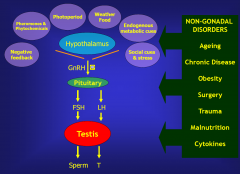
GnRH HPA
|
|
|
|
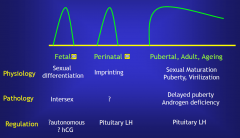
3 Epochs of Testicular Testosterone Production
|
|
|
|
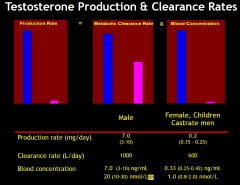
Testosterone Production & Clearance Rates
|
|
|
|
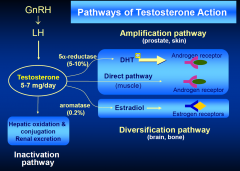
PAthways of Testosteron action
|
|
|
|
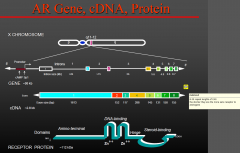
Androgen Receptor (AR) gene
|
|
|
|
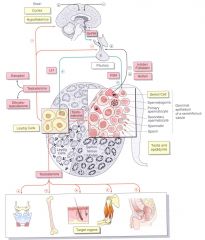
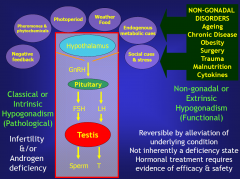
HPA and Androgens
|
|
|
|
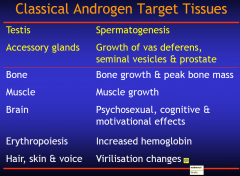
Classical Androgen Target Tissues
|
|
|
|
Androgen Deficiency
|
|
|
|
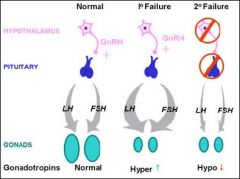
Types of Failure
|
|
|
|
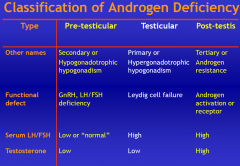
Classification of Androgen Deficiency
|
|
|
|
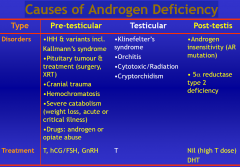
Causes of androgen def.
|
|
|
|
Clinical Features of Androgen Deficiency
History |
• General medical history
• Clinical context (delayed puberty, infertility, poor virilisation), reproductive toxins, occupation • Developmental • Cryptorchidism, torsion, inguinal hernia, timing & tempo of puberty, virilization, family history • Reproductive history • Marital & fertility status, sexual function, STI • Underlying disease • Headache, visual disturbance, olfaction, pigmentation, obesity, depression • Non-specific symptoms • Changes in well-being, energy & vitality, lethargy, fatigue |
|
|
Clinical Features of Androgen Deficiency
Physical Examination |
• General
• Olfaction, mid-line facial defects (Idiopathic hypogonadotrophic hypogonadism) • Visual fields (Pituitary tumour) • Peripheral vessel pulses & leg reflexes (Erectile function) • Virilization • Eunuchoidal, body hair, voice, musculature, gynecomastia, acne • Genital examination • Testis volume ± atrophy • Hypospadias, cryptorchidism, inguinal surgery, • Vas & epididymis orcodomitor - testicular exam - clinfeed syndrome 47XXY - small testies -75% go through life unDx |
|
|
Clinical Features of Androgen Deficiency
Investigations |
• Hormone assays
Routine • Total testosterone – two samples, different mornings • LH, FSH, SHBG (routine) Selective • Prolactin, α subunit, thyroid function (TSH), IGF-I, cortisol • DHT, estradiol, DHEA(S), 17 hydroxyprogesterone, • hCG or GnRH stimulation tests (rarely needed) • Other tests for diagnosis or pre-treatment Routine • Bone density, PSA, hemoglobin Selective • Genetics - karyotype (Klinefelter’s), Y chromosome microdeletion • Hypothalamus & pituitary radiology (CT, MRI) • Iron studies (transferrin saturation, HFE C282Y genotype) • Semen analysis (fertility) |
|
|
Klinefelter’s Syndrome
|
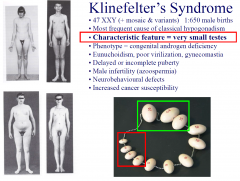
• 47 XXY (+ mosaic & variants) 1:650 male births
• Most frequent cause of classical hypogonadism • Characteristic feature = very small testes • Phenotype = congenital androgen deficiency • Eunuchoidism, poor virilization, gynecomastia • Delayed or incomplete puberty • Male infertility (azoospermia) • Neurobehavioural defects • Increased cancer susceptibility |
|
|
Kallmann’s Syndrome
|
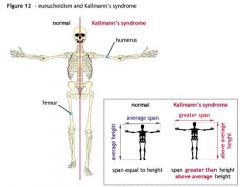
• Idiopathic hypogonadotrophic hypogonadism (IHH)
• Kallmann’s = IHH + anosmia (mid-line facial defects) • Rare (1:10-25,000 births) • Phenotype = congenital androgen deficiency • Eunuchoidism, poor virilization, gynecomastia • Present with delayed or incomplete puberty • Diverse gene defects identified – Kal-1, DAX-1, FGFR1, GPR54, GnRHR • Treatment with T for virilisation &/or gonadotrophins to induce spermatogenesis and fertility |
|
|
Androgen Insensitivity
|
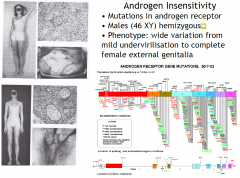
• Mutations in androgen receptor
• Males (46 XY) hemizygous • Phenotype: wide variation from mild undervirilisation to complete female external genitalia the receptor is on the X chromosome and so will express the receptor with no back up |
|
|
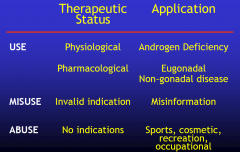
Androgen Use, Misuse & Abuse
|
|
|
|
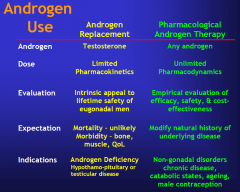
Androgen
Use |
|
|
|
Androgen Replacement Therapy:
|
Goals and Rationale
• Efficacy: To reproduce physiological levels of testosterone in blood and tissues • Safety: To replicate the life-time safety of eugonadal men Design Features • Testosterone: low oral bioavailability & rapid metabolism • Life-long treatment • Convenience = compliance = continuation • Safety, efficacy, cost, misuse potential |
|
|
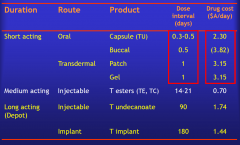
Current Testosterone Products
|
|
|
|
Androgen Replacement Therapy
Monitoring & Outcomes |
• Clinical response
• Well being & leading symptom(s) • Side-effects (mood, sexuality, sleep & product-specific) • Virilization (muscle, hair) • Compliance – continuation of treatment • Monitoring • Bone mineral density (1-2 yearly) • Prostate – PSA (baseline, annual after 50 yr) • Hemoglobin (baseline, with change of treatment) • Cardiovascular – standard risk factors (smoking, BP, lipids) |
|
|
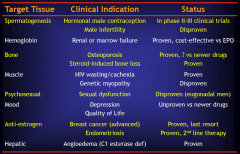
Pharmacological Androgen Therapy
|
|
|
|
Misuse of Androgens
|
•Prescribing without valid indications (reliable evidence of
efficacy & safety) •Male infertility •Sexual dysfunction without proven androgen deficiency •Non-specific symptoms without proven androgen deficiency •Older men (“male menopause” ,“andropause”, “late-onset hypogonadism”) •Women •Exact boundary is subjective but extremes such as mass marketing and promotion in absence of reliable evidence are clear •Androgens are highly susceptible to wishful marketing & promotion for sexual dysfunction or anti-ageing |
|
|
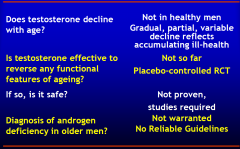
Androgens & Male Ageing
Summary of Key Issues |
|
|
|
Misuse of Androgens
- ve effects |
•Potential harmful effects
Risk of accelerating cardiovascular or prostate disease Contrary to rational, evidence–based prescribing •Highly susceptible to marketing promotion Lay & media images of “male sex hormone” Wishful thinking about anti-ageing Rejuvenation for the wealthy, worried well Exploitation by commercial entrepreneurs: pharmaceutical industry franchised and single-issue clinic •Responsible use of “off-label” prescribing Self-regulated therapeutic freedom vs restrictive independent legal regulation |
|
|
Abuse of Androgens
|
• Definition: Illicit use of androgens without medical indication or
prescription • Motives: Elite power sports, cosmetic, recreational or occupational • Sources: Underground black-market fed by illicit manufacture, thefts and diversion from legitimate agricultural, veterinary & medical suppliers • Risks: Increased cardiovascular and prostate disease plus reproductive dysfunction (infertility, sexual dysfunction), hepatoxicity (liver cancer, peliosis), mood & behaviour disturbance (hypomania), shared needle risks |
|
|
Testosterone & Muscle
|
testosterone at high doses INC. muscle and strength (LINEAR)
- no upper limit the peak abuse of androgens is now over, on the decline |