Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
11 Cards in this Set
- Front
- Back

teen boy injured hip competing in a track meet. xray in Fig. Which muscles is most likely injured? 1-Tensor fascia lata; 2-Gluteus medius; 3-Gluteus minimus; 4-Rectus femoris; 5-Biceps femoris
|

Adolescent athletes may sustain an avulsion of the anterior inferior iliac spine (AIIS) which is due to the pull of the rectus femoris,Ans4
|
|

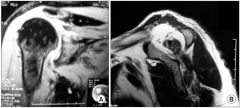
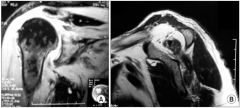
68yo F R-hand dom c/o R shoulder injury Fig, denies shoulder pain prior to a fall @ work after slipping on some water 4 wks ago, smokes 1/2 ppd. Which characteristics of this pt confer the >est risk of not healing p/surgical repair? 1-1/2 ppd smoking; 2-Surgical repair 4 wks p/injury 3-Worker's comp case; 4-68 yrs of age; 5- R-hand dom
|
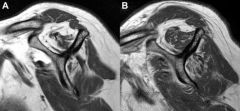
Pt age older> 65 is the highest risk factor for nonhealing of the surgically repaired rotator cuff, Advanced fatty infiltration & mus atrophy on MRI & sign glenohumeral DJD are relative contraindications for rotator cuff repair.Ans4
|
|
Which of the statements re: RCR is true? 1-Bone anchor drilling enhances vascularity p/RCR; 2-Shoulder motion p/ RCR should be restricted to enhance blood flow to repair site; 3-Doub row RCR >clinical results when compared to sing row repairs; 4-Subacr decomp > rates of succ RCR; 5-Failure to heal the RCT-> bone consistently results in poor pt outcomes
|

Suture anchor drilling into hum head has been shown to > vascularity response during RCR, peribursal tissue and bone anchor site were the main conduits of blood flow for the rotator cuff tendon. Blood flow of repaired RCT < w/time, but exercise significantly enhanced blood flow to the repaired RCT.Ans1
|
|
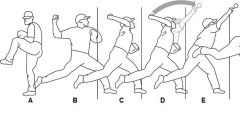
The RCT in an overhead throwing athlete is most susceptible to tensile failure due to eccentric loading during which of the phases of throwing Fig? 1-A; 2-B; 3- C; 4-D; 5-E
|
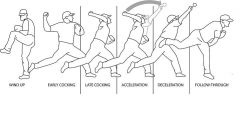
deceleration phs of throwing in the overhead athlete, the RCT is the principle decelerator of the arm, is susceptible to tensile failure due to eccentric loading during this phase.Ans5
|
|
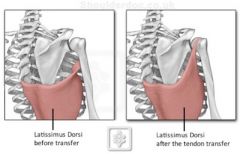
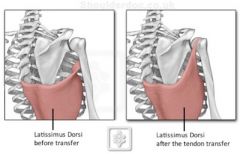
Which pt has the best indication for latissimus dorsi transfer? 1-55yo M w/ RCT arthropathy & prox hum migration; 2-85yo M w/ irreparable posterosuperior RCT & 60 deg forwd elevtn & 0 deg-active ER @ his side; 3-45yo M w/ complete irreparable supraspinatus & subscapularis tears w/ 90 deg-active forwd elevtn
4-50yo M w/large irreparable posterosuperior RCT w/100 deg-forwd elevtn & -10 deg-ER; 5-35yo w/ an acute traumatic complete posterosuperior RCT w/ 0 deg-active ER |
younger adult pt w/ an irreparable posterosuperior RCT, lack of advanced glenohumeral DJD, has an intact subscapularis function to stabilize the hum head after latissimus transfer, and who maintains some active forwrd elev.Ans4
|
|
What is the avg med-to-lat dist of the supraspinatus tendon inser @ its ftprint on the grtr tuberty? 1-6-8mm; 2-14-16mm; 3-20-22mm; 4-24-26mm;5-30-32mm
|
cadaveric have shown the avg med-to-lat dist of the supraspinatus tendon footprint on the grtr tuberity is 14-16mm/1.4-1.6 cm, measured 14.7mm, Large RCT=3-5 cm or 30-50 mm Massive > 5 cm or 50mmAns2
|
|
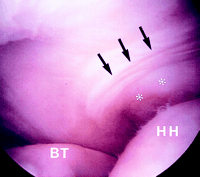
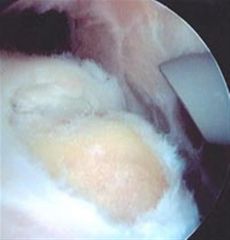
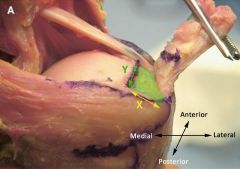
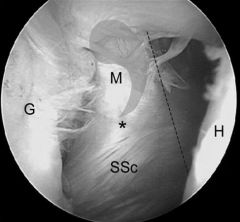
During diag scopic eval of a pt's shoulder, you ID a thickened portion of the coracohumeral lig, near its avascular zone, runng perpendicular to the supraspinatous tendn. it is in Fig w/black arrows. What is the name for this structure? 1-Mid glenohumeral lig;
2-Rotator interval; 3-Coracoid process; 4-Rotator cable 5-Rotator crescent |
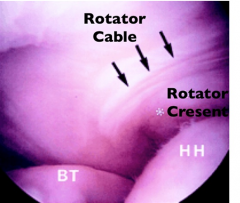
black arrows ID the rotator cable, while the asterix identifies the rotator cresent. rotator crescent & rotator cable =2 anatomic structures closely assoc w/RCT that form the shoulder's "suspension bridge." The crescent is bounded at its proximal margin by a thick bundle of fibers called the rotator cable, and thickened portion of supraspinatus.Ans4
|
|
latissimus dorsi tendn transfer is for tx of massive irreparable posterosuperior RCT. All have been shown to result in worse clinical outcomes p/transfer EXCEPT?1-Nonsynergistic action of the transferred mus; 2-Fatty atrophy of the supraspnts & infraspnts; 3-Deficien of the subscplrs; 4-Absence CA lig; 5-Deltoid weakness
|
Absence of the CA lig may allow anterosuperior escape in RC deficient shoulders BUT has NOT been shown to lead to worse outcomes p/tendon transfer, pts w/ deficiency of the deltoid/subscapularis, nonsynergistic mus action p/transfer, or fatty infiltration of the posterosuperior cuff have worse clinical outcomes.Ans4
|
|
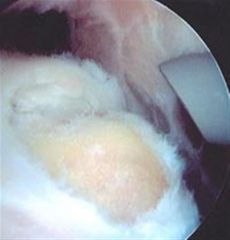
Which of the following may be seen during scopy in a pt w/subscapularis tear? 1-Uncovered lesser tub; 2-Retraction subscapularis tendn to the level of the glenoid; 3-Avulsed superior glenohumeral lig; 4-Med biceps subluxation; 5-All of the above
|
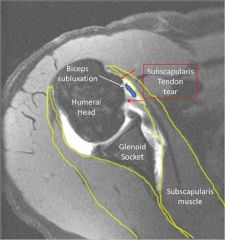
superior glenohumeral ligament(SGHL)/coracohumeral ligament(CHL) complex may show a partial tear which has been called the "comma sign", All of the findings mentioned may be encountered.Ans 5
|
|

20yo footbll player is injured, tx regimen includes immobilization of the knee in 120 deg flex. What injury has this pt most likely sustained? 1-iliac crest contsion; 2-Avulsion fx of the lesser trochanter; 3-Quadriceps contsion; 4-Hamstring rup; 5-Sports Hernia
|

Surveillance for comprtmnt synd =needed acutely & chronic manifes= myositis ossificans, Iliac crest contusions or “hip pointers” occur after direct trauma & benefit from placing the affected leg in extnsn. Athletic pubalgia or “sports hernia” is an injury to the mus of the abd wall or add longus that prod ant pelvis & groin pain in absence of a true inguinal hernia.Ans3
|
|

34yo M playing rugby 2 wks ago when an opposing player fell on the lat aspect of his L knee, felt an immediate pop & was unable to bear wt on the extremity initially, has had recurrent popping & catching in the knee since the initial injury & intermittent numb on the top of ft. xray,MRI Fig, What is the next step in management?
|

1-scopy for repair or debrid of men tear; 2-Reconst of ACL; 3-scopy for repair/debrid of femoral condyle OCD
4-CR of dislocation; 5-(EMG) for evaluation of ant tarsal tunnel synd::: CR is done by placing an appr directed force to the fibular head with the knee flexed between 80° - 110°, which relaxes the LCL & biceps fem tendn, Open red is indic for the acute dislocn that is NOT successful CR, continued instability, surg tx=arthrodesis, fib head resec, proxtibiofibular jt capsule recon.Ans4 |