Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
152 Cards in this Set
- Front
- Back
|
Miller's Recession Classification
Class I (2) |
Recession coronal to mucogingival junction.
No loss of bone/ soft tissue interdentally |
|
|
Miller's Recession Classification
Class II (2) |
Recession apical to mucogingival junction
No loss of bone/ soft tissue interdentally |
|
|
Miller's Recession Classification
Class III (2) |
Recession at or beyond mucogingival junction
Loss of interdental tissue coronal to marginal recession |
|
|
Miller's Recession Classification
Class IV (2) |
Recession at or beyond mucogingival junction
Loss of interdental tissue = marginal recession |
|
|
1999 Classification
Categories (8) |
1 - Gingival diseases (A,B)
2 - Chronic Periodontitis (A,B) 3 - Aggressive Periodontitis (A,B) 4 - As a manifestation of Systemic Disease (A,B,C) 5 - Necrotising Perio disease (A,B) 6 - Periodontal Abscess (A,B,C) 7 - Perio w/ endo lession (A) 8 - Developmental/ Acquired conditions (A,B,C,D) |
|
|
1999 Classification
Sub-classifications (classes 1,2,3) (2) |
A = Localised
B = Generalised |
|
|
1999 Classification
Sub-classifications (class 4) (3) |
4A - Haemological
4B - Genetic 4C - Others |
|
|
1999 Classification
Sub-classifications (class 5) (2) |
5A - NUG
5B - NUP |
|
|
1999 Classification
Sub-classifications (class 6) (3) |
6A - Gingival
6B - Periodontal 6C - Pericoronal |
|
|
1999 Classification
Sub-classifications (class 8) (4) |
8A - Tooth-related factors
8B - Mucogingival Deformations 8C - Mucogingival Deformations (Edentulous) 8D - Occlusal Trauma |
|
|
Recession
% of pts with ≥1mm recession? |
50%
|
|
|
Recession
Epidemiology (2) |
M>F
Buccal most common |
|
|
Recession
Aetiology (10) |
Developmental Absence
Frenal pulls Piercings Habits Disease Smoking Orthodontic Rx Abrasion Dentures Malocclusion |
|
|
Miller's Mobility Index
Classify (4) |
0 - ≤0.2mm
I - 0.3 → 1mm II - >1mm III - vertical movement |
|
|
1989 AAP Classification
Disadvantages (3) |
Lack of gingival disease
Age based, not disease based Overlapping Categories |
|
|
1989 AAP Classification
Categories (5) |
1) Early Onset Perio (A,B,C)
2) Chronic Adult Perio (>35yo) 3) Necrotising Ulcerative Perio 4) Refractory Perio 5) Perio associated w/ systemic disease |
|
|
1989 AAP Classification
Class 1 subcategories (3) |
1A) <7yo
1B) 8-12yo 1C) 13-35yo |
|
|
Basic Periodontal Exam
Changes in adolescents? (3) |
Quadrants not sextants
Only central incisors and first molars used Only in children >12yo |
|
|
Periodontal Probes
CPTIN Probe Acronym stands for? |
Community Periodontal Treatment Index Need
|
|
|
Periodontal Probes
CPTIN Probe Alternative name? |
WHO probe
|
|
|
Periodontal Probes
CPTIN Probe Markings and tip? (3) |
Ball end (0.5mm)
3.5→5.5mm = black 8.5→11.5 = black |
|
|
Periodontal Probes
CPTIN Probe Use? |
BPE
|
|
|
Periodontal Probes
CP12 Probe Markings and tip? |
Blunt end
3→6mm = black 9→12mm = black |
|
|
Periodontal Probes
CP15 Probe Difference from CP12 Probe? |
Extra marking at 15mm length
|
|
|
Periodontal Probes
TPS Probe Benefit over CP12 Probe? |
Markings to show correct probing force
|
|
|
Periodontal Probes
Which type is electronically pressurized, very accurate and mostly used for research? |
Florida Probe
|
|
|
Root Surface Instrumentation
Indications? (4) |
True Pockets
PD ≥4mm BoP Adequate Oral Hygiene |
|
|
Root Surface Instrumentation
Outcome |
Long Junctional Epithelium
(Epithelial cells with hemi-desmosomal attachments to root surface) |
|
|
Root Surface Instrumentation
Benefits of successful treatment? (3) |
Less inflammation
Gain in attachment Improved tissue resistance |
|
|
Root Surface Instrumentation
Rate of epithelial re-attachment? |
~1mm day⁻¹
|
|
|
Bleeding on Probing
% of sites which progress to LOA? |
30%
|
|
|
Bleeding on Probing
Why is this used as an indicator of disease? |
95% of sites w/o BoP do not progress to LOA
|
|
|
Loss of Attachment
Define |
ACJ ↔ Base of pocket
|
|
|
Gingivitis
Clinical finding |
No LOA but ↑PD
|
|
|
Periodontal Probes
Probe used for detecting subgingival calculus? |
Cross Calculus Probe
|
|
|
Dentine Hypersensitivity
Presenting complaint (3) |
Short, sharp pain
May be episodic Can be spontaneous or in response to stimuli resulting in a fluid outflow from tubules |
|
|
Dentine Hypersensitivity
Diagnostic Criteria (2) |
Symptoms fit
Other pathology excluded |
|
|
Dentine Hypersensitivity
Epidemiology (3) |
~15% of population
F>M (and younger) 20-50yo |
|
|
Dentine Hypersensitivity
Teeth most commonly affected (6) |
3, Canines
4, First Premolars 1, Central Incisors 2, Lateral Incisors 5, Second Premolars 6,7,8 Molars |
|
|
Dentine Hypersensitivity
Surface most commonly affected |
Buccal Cervical
|
|
|
Dentine Hypersensitivity
Causes of dentinal exposure (5) |
Attrition
Abrasion Abfraction Erosion Periodontal Disease |
|
|
Dentine Hypersensitivity
Absi et al's SEM results (2) |
Sensitive dentine has 8x the number of open tubules
Open tubules had double the mean diameter |
|
|
Dentine Hypersensitivity
Current theory of dentinal pain conduction? |
Hydrodynamic theory
|
|
|
Dentine Hypersensitivity
Does all exposed dentine cause pain? Why? (3) |
No
Unknown but potentially due to smear layer or CaPO₄ deposits Evidence to suggest size and number of open tubules is important |
|
|
Dentine Hypersensitivity
Two main categories of treatment? |
Inhibition of sensory nerve activity
Tubule Occlusion |
|
|
Dentine Hypersensitivity
Indirect action of treatments containing K⁺ ions (2) |
K⁺ stimulates NO release from odontoblasts
NO exerts an analgesic effect on the Aδ fibers |
|
|
Dentine Hypersensitivity
Why is K⁺ now thought to work indirectly rather than directly in nerve inhibition? (4) |
K⁺ requires direct contact with the nerve
K⁺ ions would need to travel against the fluid flow NO is freely diffusible NO can produce effects at greater distances from the nerve |
|
|
Dentine Hypersensitivity
Tubule Occlusion Treatments (4) |
Di-potassium Oxalate 30% (Sensitrol)
Silica abrasion (Toothpastes) Resins/ GI (Seal & Protect) F⁻ Varnishes (Duraphat) |
|
|
Dentine Hypersensitivity
Dietary and toothbrushing advice (3) |
Reduce acid
Brush teeth 30 mins prior to eating Ensure correct brushing force and technique |
|
|
Sensitrol
Active agent |
30% Di-potassium Oxalate
|
|
|
Sensitrol
pH |
4.3
|
|
|
Sensitrol
POI (Post Op Instruction) |
Avoid acid for 24h
|
|
|
Sensitrol
Mode of action (2) |
Tubule Occlusion
Calcium Oxalate crystal formation |
|
|
Dentine Hypersensitivity
Management of generalised hypersensitivity (3) |
Dentifrice advice
Dietary prevention F⁻ Mouthwash OD |
|
|
1999 AAP Classification
Is periodontal disease secondary to poorly controlled diabetes class IV? |
No - diabetes is a modifier of periodontal disease
|
|
|
Recession
How does a frenal pull contribute to localised recession? (2) |
Impedes plaque removal
Directly pulls tissue away |
|
|
Recession
What tissue biotype is most likely to exhibit recession? |
Type 1
|
|
|
Recession
How does smoking affect recession? |
It increases, even when there's no periodontal disease
|
|
|
Antibiotics
What does LDA stand for? |
Locally Delivered Antimicrobials
|
|
|
LDA in Periodontics
Are these a stand-alone treatment? |
No, only as an adjuct
|
|
|
LDA in Periodontics
Indications (4) |
Long standing lessions
Deep pockets Failure to respond to Rx [non-surgical] Adequate OH |
|
|
LDA in Periodontics
Ideal properties as defined by Goodson et al. 1985 (3) |
1) Must reach the base of pocket
2) Must deliver biologically active concentrations 3) Must maintain the concentration for sufficient time |
|
|
LDA in Periodontics
Depth of pocket after which mouthwashes do not reach? |
>5mm
|
|
|
LDA in Periodontics
Does CHX irrigation with a syringe reach the base of pockets? |
Not predictably
|
|
|
LDA in Periodontics
Increase in concentration required to affect a biofilm compared to planktonic bacteria? |
500x
|
|
|
LDA in Periodontics
Advantages compared to systemic? |
Site Specific.
Locally high concentrations. Prolonged exposure with slow release systems. Lower systemic side effects.(Low plasma concentration.) High patient compliance. Lower risk of super-infection. |
|
|
LDA in Periodontics
Main categories of drug? (3) |
Chlorhexidine (Antiseptic)
Tetracyclines (Bacteriostatic antibiotic) Metrinidazole (Bacteriocidal antibiotic) |
|
|
LDA in Periodontics
Constituents? (2) |
Active ingredient
Carrier |
|
|
LDA in Periodontics
Tetracycline Overview (3) |
Broad Spectrum
High resistance (~25%) Inhibits bone resorption and collagen breakdown (MMP and PMN inhibition) |
|
|
LDA in Periodontics
Categories of LDA? (2) |
Antimicrobial slow release gels
Antiseptics |
|
|
LDA in Periodontics
Antimicrobial slow release gels (2) |
Dentomycin (Minocycline)
Elyzol Dental Gel (Metronidazole) |
|
|
LDA in Periodontics
Antiseptic Preparations |
PerioChip (Chlorhexidene)
Chlo-site (Chlorhexidene) |
|
|
Dentomycin
Active ingredient? |
2% Minocycline Gel
(Biodegradable) |
|
|
Dentomycin
Method of application? (3) |
Apply with syringe
3-4 applications 14 day interval ≥5mm pockets |
|
|
Dentomycin and Elyzol
Perceived disadvantage |
MIC only maintained for 12-24h
(Minimum Inhibitory Concentration) |
|
|
Elyzol
Active ingredient? |
25% Metrinidazole Benzoate Gel
(Biodegradable) |
|
|
Elyzol
Method of application and regime? (3) |
Apply with syringe
2 applications 7 days apart |
|
|
LDA in Periodontics
Why might antiseptic systems be preferable to antimicrobials? |
No risk of resistance
|
|
|
Periochip
Active ingredient and delivery mechanism? (2) |
2.5mg Chlorhexidine Gluconate
Slow release from a biodegradable cross-linked hydrolysed gelatin polymer |
|
|
Periochip
Method of application? (4) |
RSI of site
Dry site Insert chip Advise breakdown over 7-10 days |
|
|
Periochip
Why is its release profile preferable to the antimicrobial gels? (3) |
It has a two phase release
Initially ~7x MIC 24h to one week it maintains 0.6-3x MIC |
|
|
Chlo-Site
Active Ingredients? (2) |
0.5% Chlorhexidine digluconate
1% Chlorhexidine dihydrochloride |
|
|
Chlo-Site
Carrier and its benefits? (3) |
Xanthan Gel
It adheres to the gingivae Releases CHX slowly |
|
|
Chlo-Site
Why are there two forms of CHX? |
The digluconate produces high levels initially (7 days)
The dihydrochloride maintains MIC over days 7-15 |
|
|
Chlo-Site
Method of application? (3) |
RSI
Wash and dry sites (paper points) Syringe application of gel |
|
|
LDA is Periodontics
Evidence for? |
Some short term improvement but very minor
|
|
|
LDA in Periodontics
Evidence against? |
No long term improvements
|
|
|
LDA in Periodontics
Disadvantages? (3) |
Expensive
No long term gain Potentially systemic effects |
|
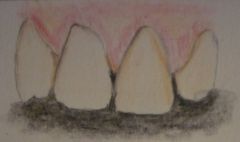
Recession
What biotype is this and what are its features? (4) |
Biotype 1
Long Papillae Thin and scalloped gingivae Predisposed to dehiscence and fenestrations Susceptible to recession |
|

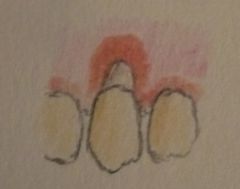
Recession
What biotype is this and what are its features? (3) |
Short papillae
Thick and flat gingivae Resistant to recession |
|

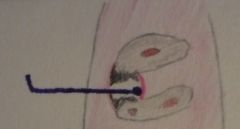
Recession
Which precursor to recession is shown? |
A Stillman's Cleft
|
|
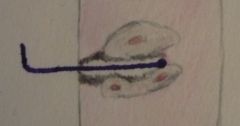
Recession
Which precursor to recession is shown? |
A McCall's Festoon
('rolled up' or swollen gingivae) |
|
|
Recession
Treatments (2) |
S&P/ RSI (Prevent further)
Mucogingival Surgery |
|
|
Recession
Methods of monitoring progression? (3) |
Serial Photographs
Serial Study Models Recording of PD and LOA |
|
|
Furcation Involvement
Can a radiograph diagnose furcation involvement? |
No, the diagnosis is clinical.
|
|
|
Furcation Involvement
Why does this reduce the tooth's prognosis? (2) |
Harder to clean
May result in loss of vitality (accessory canals) |
|
|
Furcation Involvement
Rx for Hamp Class I Lesion? (3) |
S&P
RSI Furcationplasty |
|
|
Furcation Involvement
Rx for Hamp Class II lesions? (6) |
Furcationplasty
Tunnel Preparation Root Resection XLA GTR EMD |
|
|
Furcation Involvement
Rx for Hamp Class III lesions? (3) |
XLA
Tunnel Preparation Root resection |
|
|
Furcation Involvement
Furcationplasty procedure (5) |
Raise flap
Remove granulation tissue RSI Odontoplasty Osteoplasty |
|
|
Furcation Involvement
How does a furcationplasty differ from a tunnel preparation? |
Tunnel preparations aim to leave the defect cleanable, furcationplastys aim to close the defect.
(query answer) |
|
|
Furcation Involvement
Complications of furcationplasty/ tunnel preparation? (3) |
Loss of vitality
Root caries Hypersensitivity |
|
|
Furcation Involvement
Root Resection Procedure (4) |
RCT within 2 weeks (ideally before)
Retain most stable root when possible Surgically remove resected root Retrograde fill defect |
|
|
Furcation Involvement
Hamp Classification I |
Horizontal loss ≤⅓ tooth width
|
|
|
Furcation Involvement
Hamp Class II |
Horizontal loss >⅓ <1 width of tooth
|
|
|
Furcation Involvement
Hamp Class III |
Complete horizontal loss of tissues.
|
|
|
Akerly Classification
Class I |

Lower incisors impinge on palatal mucosa
|
|
|
Akerly Classification
Class II |

Lower incisors impinge on palatal gingival margins
|
|
|
Akerly Classification
Class III (2) |

Lower incisors impinge on palatal gingival margins
Upper incisors impinge on lower labial gingival margins |
|
|
Akerly Classification
Class IV |

Lower incisors occlude with palatal surface of upper incisors
|
|
|
Perio Treatment Planning
5 phases in Perio (5) |
1) Initial exam & Pain relief
2) Cause related therapy (Clinical checks, advices and hands-on therapy) 3) Re-examination 4) Definitive treatment 5) Maintenance |
|
|
Perio Treatment Planning
At re-examination pt has ≤3mm PD and no BoP - next stage? |
Maintenance
|
|
|
Perio Treatment Planning
At re-examination pt has >3mm PD and BoP - next stage? (3) |
Determine cause
If treatable cause then phase 4 (Definitive Rx) If not then palliative care |
|
|
Perio Treatment Planning
At re-examination pt has >3mm PD but no BoP - next stage? |
Review in 1/12 (Likely a slow healer)
|
|
|
Perio Treatment Planning
Which stage for cured pts? |
Trick question - can't cure perio disease
|
|
|
Periodontal Palliative Care
Usual treatment plan? |
3/12 S&P
|
|
|
Perio Treatment Planning
Factors affecting phase 5 recalls (2) |
General risk factors
Local risk factors |
|
|
Susceptibility to Periodontitis
Factors? (4) |
Age
Oral hygiene levels Severity of disease Relationship of plaque scores to BoP |
|
|
Perio Treatment Planning
General factors affecting prognosis? (6) |
Type of disease
Susceptibility Systemic health Treatment required Oral hygiene Availability for Rx |
|
|
Perio Treatment Planning
Local factors affecting prognosis? (6) |
Degree of restorations
Crowding of teeth Anatomy of teeth Furcation involvements Recession Appliance wear |
|
|
Enamel Matrix Derivative
Trade name? |
Emdogain
|
|
|
Enamel Matrix Derivative
Active ingredients (2) |
Porcine derived
Amelogenins + other related proteins |
|
|
Enamel Matrix Derivative
Indications for use (3) |
1,2,3 wall defects
Hamp II furcations ≥6mm PD and >3mm radiographic LOA |
|
|
Enamel Matrix Derivative
Storage and pre-operative care (4) |
Store refrigerated
0.3ml/0.7ml syringes Warm for 30mins pre-op Use within 2 hours |
|
|
Enamel Matrix Derivative
Procedure (8) |
0.12% CHX for 1 min
LA Raise flap RSI 'Root surface bio-modification' Saline rinse Place EMD Close flap |
|
|
Enamel Matrix Derivative
What is 'Root surface bio-modification'? (4) |
Removal of the smear layer by;
Citric Acid (pH1)/ Phosphoric acid (15s)/ 24% EDTA gel (pH6.7 for 2 mins) |
|
|
Enamel Matrix Derivative
Post op instruction (4) |
Paracetamol/ Ibuprofen if painful
CHX MW 2x daily No mechanical cleaning for 3 weeks No inter-proximal cleaning for 6 weeks |
|
|
Enamel Matrix Derivative
Antibiotic use? (3) |
21 days of 100mg doxycycline
Begin one day pre-op At clinician's discretion |
|
|
Enamel Matrix Derivative
Pharmokinetics (6) |
Binds to hydroxyapatite and collagen
Coagulin fills defect Carrier disappears after 12-24h Days) Mesenchymal cells attach Weeks) New CT develops Months-Year) Resolution of defect |
|
|
Enamel Matrix Derivative
Where does new bone formation begin? |
At the treated root surface
|
|
|
Enamel Matrix Derivative
Post operative supervision (3) |
Bi-monthly recall for 6/12
6/12 to 1 year 3/12 recall S&P and OHI as required |
|
|
Systemic Antimicrobials
Use in Refractory periodontal disease? |
Not indicated
|
|
|
Systemic Antimicrobials
Adjunct to ANUG treatment dosage? (4) |
Metrinidazole
200mg tds 3 days |
|
|
Systemic Antimicrobials
Use in NUP? |
Indicated but no clear protocol
|
|
|
Systemic Antimicrobials
Adjunct to Ag Periodontitis treatment? (4) |
Amoxicillin 250mg
Metrinidazole 400mg tds 7 days |
|
|
Systemic Antimicrobials
Dosage for perio abscess without drainage? (4) |
Amoxicillin
250mg tds 5 days |
|
|
Periostat
What is Periostat? (4) |
Doxyciclin Hyclate 20mg
Sub-antimicrobial concentration Taken bd 1 hour before food 3 month regimes, max 9 months |
|
|
Periostat
Mode of action? |
Inhibits Collagenases (Matrix Metalloproteinase enzymes)
|
|
|
Periostat
Effects? (3) |
Reduces collagen breakdown
Promotes repair and healing Inhibits disease progression |
|
|
Periostat
Evidence for? |
Yes, ↓PD + ↑reattachment
Rebound effect can occur More research required |
|
|
Periostat
Indication |
Generalised severe periodontitis
|
|
|
Periostat
Contra-indications (3) |
Allergy to Tetracyclines
Pregnancy / Breast-feeding Children < 12 years old. |
|
|
Periostat
Warnings and interactions (4) |
Warfarin (~↑INR)
Penicillin Oral contraceptives Photo-sensitivity |
|
|
Guided Tissue Regeneration
Ideal barrier properties (5) |
Inert and bio-compatible
Act as a barrier to epithelial invasion Allow tissue integration Maintain space Easily shaped, placed and trimmed |
|
|
Guided Tissue Regeneration
Most common barrier material |
Expanded Polytetraflourethylene
(e-PTFE) |
|
|
Guided Tissue Regeneration
Procedure (5) |
Raise flap
Thorough RSI Membrane placed (>3mm extensions) Suture Remove membrane after 4-6 weeks |
|
|
Guided Tissue Regeneration
Post-op instruction (3) |
Avoid brushing site for 3 days
0.2% CHX MW for 4-6 weeks Antibiotics 1-2 weeks |
|
|
Guided Tissue Regeneration
Factors affecting outcomes (Patient) (4) |
Smoker/ non-smoker
Plaque score <15% Bleeding score <15% Smaller bone defects |
|
|
Guided Tissue Regeneration
Factors affecting outcomes (Operational) (3) |
Correct membrane placement (no exposure)
Adequate flap Flap design (Modified Papilla Preservation Technique [MPPT] is advised) |
|
|
Periodontal Surgery
Contra-indications (5) |
Bleeding disorders
Significantly immunocompromised Uncontrolled systemic disease Smoking Poor co-operation |
|
|
Periodontal Surgery
Procedures (6) |
Gingivectomy
EMD GTR Root resection RSI Crown lengthening |
|
|
Splints
3 types of fixed splints |
Composite bonded
Orthodontic wire Resin retained |