Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
describe LYMPHOCYTES and their function; give examples
|
Lymphocytes-responsible for antibody production and cellular immunity
occur in blood, lymphatic circulation, spleen T-cells B-cells Natural killer cells |
|
|
describe PHAGOCYTES and their function; give examples
|
Two main classes of phagocytes:
Monocytes Granulocytes --Neutrophils-first response, pus --Eosinophils-allergic rxn, parasites --Basophils-allergic and antigen response, histamine prod = inflam |
|
|
describe AGRANULOCYTES and their function; give examples
|
Agranulocytes: Agranulocytes are a category of white blood cells characterised by the absence of granules in their cytoplasm; they include: Lymphocytes
Monocytes |
|
|
describe MONOCYTES and their function
|
Monocytes which migrate from the bloodstream to other tissues will then differentiate into tissue resident macrophages or dendritic cells
|
|
|
describe the (3) types GRANULOCYTES and their function; give examples
|
Neutrophil:
-First responders -motile (attracted by cytokines) -hallmark of acute infections -phagocytic (killing by “respiratory burst”: highly reactive oxygen species in phagolysosome) in PUS -Granules: Primary (promyelocytic stage) and secondary (predominant in mature neutrophil: collagenase, lactoferrin, lysozyme) Basophils: only occasionally seen in peripheral blood -allergic and antigen response via histamine causing inflammation. -Granules: contain heparin (anticoagulant) and histamine (vasodilation) Eosinophils: special role in allergic response, defense against parasites (helminths), removal of fibrin formed during inflammation Acidic granules contain: peroxidase, RNase, DNases, lipase, plasminogen Degranulation is toxic to invaders but also to host |
|
|
Understand the naming and staining pattern of the granulocytes.
|
Neutrophils - Neutral PINK color
Basophils - DARK BLUE cellular components, stain with the basic dye hematoxylin Eosinophils - Bright RED cellular components, stain with eosin |
|
|
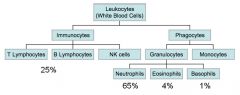
Know which of the leukocytes are more common.
|
N > E > B
"ben backwards' |
|
|
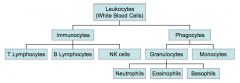
Draw the "tree" of leukocytes to sort out which is which, annotate it as necessary for understanding and which types are most/least common.
|
|
|
|
Draw the "tree" of leukocytes to sort out which is which, annotate it as necessary for understanding and which types are most/least common.
|
|
|
|
Understand what band and segs are and their importance for clinical diagnosis.
|
Band neutrophils (stabs): immature neutrophils (immature rod-like nucleus) (increased in patients with infections/inflammations)
Segmented neutrophils: mature neutrophils (segmented nucleus) |
|
|
Know what monocytes and macrophages are and their tissue distribution.
|
Monocytes are present in blood and mature to macrophages in tissues (tissue-specific macrophages)
|
|
|
Describe the (3) types of lymphocytes
|
T-cells: develop from cells that have migrated to thymus, cellular immune response
B-cells: antibody producing cells (humoral immune response), mature in bone marrow, circulate in peripheral blood & lymphatic circulation until recognition of antigen Natural killer cells:Kill tumors and virus-infected cells by releasing contents of granules (induce apoptosis) |
|
|
Know what reticuloendothelial system stands for.
|
The phagocytic system of the body, including the macrophages of tissues, liver and spleen, primarily monocytes and macrophages
|
|
|
Understand the two important functions of the spleen as a ____ ____ and as part of the ____ system.
|
blood filter , immune
|
|
|
Know what the red pulp and white pulp are responsible for.
|
Red pulp: 75% of spleen, Red blood cell monitor
White pulp: Lymphocytes, macrophages, dendritic cells |
|
|
Remember that the ____ and ____ can become hematopoietic (extramedullary) in extreme circumstances.
|
Spleen, liver
|
|
|
Be able to briefly define splenomegaly and hypersplenism.
|
Splenomegaly - ENLARGEMENT of spleen due to a large variety of conditionsHypersplenism -Increased spleen FUNCTION
|
|
|
Know what leukopenia and leukocytosis mean (understand the suffix –penia and –cytosis) and be able to rationalize what conditions could lead to those.
|
Leukopenia - low WBC from:
-Bone marrow failure (for example, due to infection, tumor, or abnormal scarring) -Collagen-vascular diseases (such as lupus rythematosus) -Disease of the liver or spleen -Radiation Leukocytosis - high WBC from: -Anemia -Infectious diseases-Inflammatory disease (such as rheumatoid arthritis or allergy)-Leukemia -Severe emotional or physical stress -Tissue damage (for example, burns) |
|
|
What is respiratory burst?
|
rapid release of reactive oxygen species (superoxide radical and hydrogen peroxide) from different types of cells.
|
|
|
Be familiar with the terminology of the different assays in the complete blood count. In other words look over these and make sure you understand them:
White blood cell count White blood cell differential (distinguishes between the different types of white blood cells) Red blood cell count Hemoglobin Hematocrit Mean corpuscular volume (MCV) Mean corpuscular hemoglobin (MCH) Mean corpuscular hemoglobin concentration (MCHC) Platelet count |
na
|
|
|
Be able to define leukemia, lymphoma, and myeloma.
|
Leukemia: Overproduction of immature cancerous white blood cell precursors, originating in bone marrow (causes bone marrow failure, neutropenia, anemia, infiltration of other organs), causes neutropenia b/c crowd out other cells
Myeloma:Cancer of plasma cells (B cells) in bone marrow (decreased immune function, eventually myeloma cells invade other parts of body) Lymphoma: Cancer of lymphocytes in lymph nodes (occasionally entering bloodstream) |
|
|
Be able to briefly outline the general progression of leukemia.
|
Disease originates in bone marrow-> spleen, lymph nodes and liver
|
|
|
What is chronic leukemia?
|
Chronic - Aggressively proliferating malignant blast cells (hematopoietic stem cell)
CLL: chronic lymphoid leukemia -several disorders affecting B- or T-cells -most common type of leukemia -no cure, but often slow progression CML: chronic myeloid (myelogenous) leukemia -WBC cancer caused by philadelphia chromosome translocation |
|
|
What is acute leukemia?
|
Acute - rapidly proliferating malignant blast cells, curable
|
|
|
What is lymphotic leukemia?
|
Lymphocytic
Cancer where lymphocytes proliferate abnormally Accumulation of white cells in the lymph nodes (only occasionally entering blood or extra-lymphoid tissue in later “leukemic phase”)lym- -Hodgkins = involves the Reed-Sternberg cells (giant B cells), Epstein Bar virus, high cure rate (60-90%) -non-Hodgkins = No Reed-Sternberg cells involved , B or T -cell involved |
|
|
What is myeloid leukemia?
|
Cancer of plasma cells in bone marrow (decreased immune function, eventually myeloma cells invade other parts of body)
|
|
|
Be able to define Hodgkin’s and non-Hodgkin's lymphoma. Know what a Reed-Sternberg cell is.
|
-Hodgkins = involves the Reed-Sternberg cells (giant B cells), Epstein Bar virus, high cure rate (60-90%)
-non-Hodgkins = No Reed-Sternberg cells involved , B or T -cell involved |
|
|
What are the most common leukocytes?
|
Neutrophils
|
|
|
Are leukocytes derived from the lymphoid and/or myeloid cell lineage?
|
Both lymphoid (T&B) and Myeloid (Eos, basophils, macrophages, monocytes, neutrophils)
|
|
|
What are the phagocytic cells?
|
Neutrophils and macrophages
|
|
|
You suspect a patient has leukemia. Considering where the cancer originates, which laboratory test would you perform to confirm the diagnosis?
|
Bone marrow sample will be needed: aspiration/core biopsy
|
|
|
Which of the following cell types are granulocytes?
1. Basophil 2. Lymphocytes 3. Red blood cell 4. Monocytes |
choose the best answer as not all leukocytes are granulocytes!
Basophil |
|
|
What do neutrophils and macrophages have in common?
1. They are leukocytes 2. They are part of the immune system 3. They can phagocytose foreign microorganisms 4. All of the above |
all of the above, remember that the granulocytes are all phagocytic as well
|
|
|
An increased amount of band neutrophils indicates:
1. Lack of hematopoiesis 2. Increased lymphocyte count 3. Inflammation or infection 4. Increased expression of erythropoietin |
Inflammation or infection
|
|
|
Lymphocytes are derived from stem cells of:
1. the thymus. 2. the bone marrow. 3. the lymph nodes. 4. the blood. |
bone marrow
|
|
|
Hypersplenism can be caused by:
1. aplastic anemia. 2. pancytopenia. 3. surgical removal of the spleen. 4. splenomegaly. 5. All of the above |
aplastic anemia
remember megaly is a large spleen not a high functioning one. |
|
|
Leukopenia can be caused by:
1. Infections 2. Lymphoma 3. Aplastic anemia 4. Hyposplenism |
aplastic anemia also cuaed by leukemia
note that the other choices all result in leukocytosis = incr in leukocytes |
|
|
A cancer of the white blood cells originating in the bone marrow is called:
1. Erythrocytosis 2. Hodgkin's lymphoma 3. Lymphoma 4. Leukemia |
leukemia
|
|
|
ALL (acute lymphocytic leukemia) can involve which of the following cells?
1. Red blood cells 2. Platelets 3. Monocyes 4. T-cell precursors |
T-cell precursors
|
|
|
Reed-Sternberg cells are:
1. Neutrophils with segmented nuclei 2. Megaloblastic red blood cells 3. Giant white blood cells in the bone marrow 4. Giant cells derived from B-cells |
Giant cells derived from B-cells
|
|
|
The term thrombocytes refers to:
|
Platelets
|
|
|
What are the roles of ADP and thromboxane A2?
1. They are platelet activating factors 2. They convert fibrinogen to fibrin 3. They stimulate tissue factor expression 4. They inhibit blood clot formation |
They are platelet activating factors
|
|
|
Which of the following factors is a component of the common pathway (coagulation cascade)?
1. Factor VIIa 2. Factor X 3. Christmas factor (factor IX) 4. Tissue factor 5. All of the above |
Factor X
|
|
|
The Prothrombin time (PT) test is specific for:
1. Only the common pathway 2. The intrinsic and common pathway 3. The extrinsic and common pathway 4. The extrinsic, intrinsic and common pathway |
The extrinsic and common pathway
|
|
|
Several blood tests have been performed for a patient. The platelet count, platelet function tests and thrombin time are normal but the Activated Partial Thromboplastin Time (PTT or aPTT) is very slow. Which disease do you suspect?
1. Hemophilia A 2. Anemia 3. Sideroblastic anemia 4. Von Willebrand disease |
Hemophilia A
|
|
|
Plasmin, derived from plasminogen, is responsible for:
1. Activation of thrombinogen 2. Activation of fibrinogen 3. Degradation of fibrin 4. Platelet aggregation |
Degradation of fibrin
|
|
|
A deficiency in von Willebrand factor would lead to:
1. Thrombocytopenia 2. Risk of thrombosis 3. Myeloproliferative disease 4. Increased bleeding |
bleeding
|
|
|
What is VWF and what does it do?
|
Its primary function is binding to other proteins, particularly Factor VIII and it is important in platelet adhesion to wound sites
vWF appears to play a major role in blood coagulation. vWF deficiency or dysfunction (von Willebrand disease) therefore leads to a bleeding tendency |