![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
What is PNF diagonal D1 flexion for UE? |
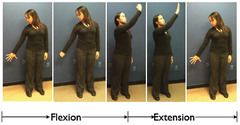
start: GH IR, ext, and ABD (throwing apple away) end: GH ER, flexion and ADD (biting apple) D1 ext is opposite Named after ENDING position |
|
|
What is PNF diagonal D2 flexion for UE? |
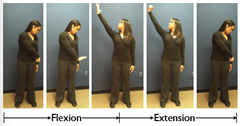
start: GH ADD, IR, ext (Drawing sword from belt) end: GH ABD, ER, flex (raising sword) Named after ENDING position |
|
|
What is PNF diagonal D1 flexion for LE? |

start: hip ABD, IR, ext
End: hip ADD, ER, and Flexion (Piriformis stretch position) D1 ext is opposite Named after ENDING position |
|
|
What is PNF diagonal D2 flexion for LE? |

start: hip ADD, ext, ER end: hip ABD, flexion, IR (W-sit position) Named after ENDING position |
|
|
What are head and trunk diagonal patterns used for? |
to enhance breathing and movement patterns (e.g. mobility)
|
|
|
What are PNF patterns incorporating trunk and neck movements? |
Chop (D1 into ext) Reverse chop (D1 into flex) Lifts (D2 into flex) Reverse lifts (D2 into ext) -supine lower trunk flexion with rotation to right or left and knees flexing for rolling and bed mobility -LE D1 flexion helps rolling in any direction
|
|
|
What is PNF chop and reverse chop? |
Chop = (Bilat. asymmetrical UE ext with trunk and neck flexion and rotation) = D1 ext with lead arm and assist arm grabs on dorsal side of wrist (use if rolling toward lead arm's side) (pg. 31 in small O'sullivan book/neuro book)
Reverse chop = Bilat asymmetrical UE flexion with neck ext and rotation = opposite of chop D1 extension (use if moving/rolling to side opp to side performing the diagonal) CHOP = D1
|
|
|
What is PNF lifts and reverse lifts? |
Lift = (Bilat. asymmetrical UE flexion with neck ext and rotation) = D2 Flexion with lead arm and support arm grabs ventral side of wrist
Reverse Lift = Bilat asymmetrical UE ext with neck flexion and rot = opposite of lift = D2 ext LIFT = D2 |
|
|
What are agonist reversals (AR)? |

-slow isotonic shortening contraction through the range followed by eccentric lengthening contraction of the same mm groups (ex: bridging & other anti-gravity movements) Indications 1. weak postural muscles 2. inability to eccentrically control body weight during movement transitions (e.g. sitting down) |
|
|
what is PNF approximation? |
joint compression indications: -used to facilitate extensor/stabilizing muscle contraction and stability -to stimulate afferent nerve endings |
|
|
what is PNF contract-relax (CR) and indications? |

-isotonic movement in rotation to range limitation followed by isometric hold of the antagonist (range limiting muscles) and then isotonic contraction of antagonist against resistance then relaxation and active movement into the new range of the agonist pattern Indications: limited range of motion caused by muscle tightness or spasticity |
|
|
what is PNF Hold-Relax (HR)? |

Isometric contraction of antagonist against resistance followed by voluntary relaxation and passive movement into the newly gained range of the agonist indications: limited ROM due to muscle tightness, spasm or pain |
|
|
What is PNF repeated contractions (RC)? |
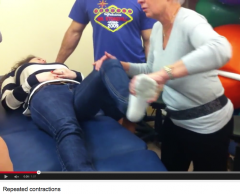
Repeated isotonic contractions induced by quick stretches and enhanced by resistance performed through the range or part of range at a point of weakness indications: weakness, incoordination, muscle imbalances and lack of endurance |
|
|
What are PNF rhythmic initiations (RI) |

voluntary relaxation followed by passive movement through increasing ROM, followed by active assisted contractions progressing to resisted isotonic contractions Indications: spasticity, rigidity, hypertonicity, inability to initiate movement (apraxia), motor learning deficits, communication deficits (aphasia) ex: 1. "relax, let me move you" 2. progress to "now, help me move you. 3. then progress to light resistance "Now, push up." 4. at end ask pt to move indep |
|
|
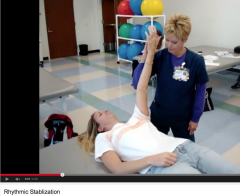
What are PNF Rhythmic stabilizations (RS)? |
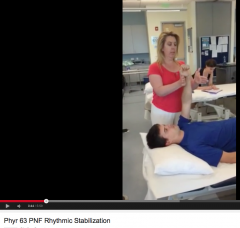
Simultaneous isometric contractions of both agonist and antagonists patterns performed without relaxation using careful grading of resistance -co-contraction of opposing mm groups Indications 1. instability in weight-bearing and holding 2. poor anti-gravity control 3. weakness 4. ataxia 5. limited ROM caused by mm tightness 6. Painful muscle splinting |
|
|
What is PNF slow reversal? |

aka Dynamic Reversals alternating isotonic contractions of agonist then antagonist patterns using careful grading of resistance and optimal facilitation Slow Reversal Hold (SRH) = isometric hold added to end of range at a point of weakness Indications: 1. inability to reverse directions, 2. muscle weakness or imbalance 3. incoordination 4. lack of endurance |
|
|
What are PNF stabilizing reversals? |
alternating isotonic contractions of first agonists and antagonists against resistance allowing only very limited movement. -technique progressses to stabilizing holds (alternating isometrics) command = Don't let me push you Indications: 1. impaired strength 2. impaired stability and balance 3. impaired coordination |
|
|
What is PNF traction? |
separation of joint surfaces Indications: facilitates flexor muscles mobilizing patterns (e.g. stretch of joint capsule and other mob indications) |
|
|
What are facilitation techniques? |
1. repetitive brushing. facilitates tactile receptors and movement responses 2. quick icing for muscles 3. quick stretch or tapping of agonist tendon or muscle belly 4. High-frequency vibration 50-3000 Hz to agonist *Facilitation techniques to antagonist inhibit agonist via reciprocal inhibition |
|
|
what are inhibition techniques? |
1. prolonged icing inhibits muscle 2. neutral warmth. relaxation by wrapping in towels or blankets to decr postural tone 3. prolonged stretch. muscle tone decreased 4. low freq vibration (5-50 Hz) 5. Pressure on tendons (firm and constant)
|
|
|
What vestibular stimulation techniques can be used for inhibition? |

slow rocking, rolling on ball inhibits postural tone |
|
|
What vestibular stimulation technique facilitates tone? |

fast spinning facilitates postural tone promotes head righting |
|
|
What can prone over large ball promote? |

vestibular stimulation -can activate postural extensors of neck, trunk and proximal joints -soothing effect for sympathetic responses |
|
|
What principles are advocated by NDT,Bobath? |
1. Motor learning (relearning) occurs through repetition and experience in the environment 2. inhibition of unwanted activity precedes practice of normal motor patterns 3. Guided movements or assisted movements only when needed. (usu early in rehab process) 4. Normalization of postural tone -inhibit reflexes -increase tone if hypotonic -decrease tone if hypertonic 5. normalization of sensory/perceptual experiences 6. resumption of functional activities that are meaningful, goal oriented 7. validity of NDT has been questioned |
|
|
what is a motorPROGRAM? |
a set of prestructured muscle commands that, when initiated, results in the production of a coordinated movement sequence |
|
|
what is a motor PLAN? |
overall strategy for movement -action sequence requiring coordination of a number of motor programs |
|
|
What is feedforward? |
sending of afferent signals in advance of movement to ready the system -anticipatory responses in postural activity |
|
|
What is feedback? |
afferent info sent by various sensory receptors to motor control centers to shape ongoing movement or allow for adaptation of motor responses Types of Feedback: 1. Intrinsic: sensory information normally acquired during performance of a task 2. Augmented: externally presented feedback that is added to that normally acquired during task performance 3. KR (knowledge of results): augmented feedback about the outcome of a mvmt 4. KP (knowledge of performance): augmented feedback about the nature of the movement produced |
|
|
What is motor skill acquisition? |
behavior is organized to achieve a goal-directed task |
|
|
what is motor learning? |
the change in the ability to perform a skill -the result of practice or experience |
|
|
what are measures of motor learning? |
1. Performance (of the skill or task) 2. Retention 3. Generalizability 4. Resistance to contextual changes |
|
|
what is retention? |
the ability to demo the skill after a period of no practice |
|
|
what is generalizability? |
ability to apply what has been learned to other similar tasks |
|
|
what is resistance to contextual changes? |
ability to apply what has been learned to other environmental contexts |
|
|
what are the components of motor learning? |
1. feedback 2. practice 3. transfer |
|
|
what are the stages of motor learning? |
1. cognitive 2. associative 3. autonomous |
|
|
what is the cognitive stage of motor learning? |
develop an overall understanding of the skill through trial and error practice |
|
|
what is the associative stage of motor learning? |
refinement of the motor strategy is achieved through continued practice -concentrate on how to do the movement rather than on what to do |
|
|
what is the autonomous stage of motor learning? |
after considerable practice the motor performance becomes largely automatic |