![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
65 Cards in this Set
- Front
- Back
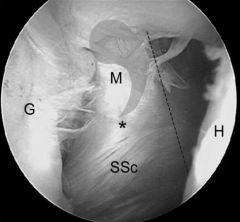
Following open pectoralis major transfer to address chronic subscapularis insufficiency, which of the following movements would most likely show weakness if an iatrogenic nerve injury occurred during the pectoralis transfer? |
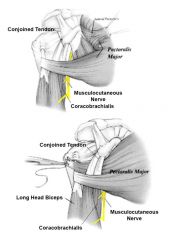
During open pectoralis major tendon transfer for chronic subscapularis deficiency, the musculocutaneous nerve is most at risk. Injury to this nerve would lead to weakness in elbow flexion.Musculocutaneous nerve neurapraxia is a known complication of the procedure caused by increased tension on the nerve. The transferred tendon should be placed deep to the conjoint tendon, but superficial to the nerve to decrease tension. A proximal musculocutaneous nerve neurapraxia could cause weakness in elbow flexion, due to its innervation of the biceps and brachialis muscles. Incorrect Answers:Answer 2: Elbow extension (triceps) is from radial nerve. Answer 3: Shoulder external rotation (infraspinatus, teres minor) is from the suprascapular and axillary nerves, respectively. Answer 4: Shoulder adduction (pectoralis major, latissimus dorsi, teres major) is from the medial and lateral pectoral nerves, thoracodorsal nerve, and lower subscapular nerve. Answer 5: Shoulder abduction (supraspinatus, deltoid) is from the suprascapular and axillary nerves.Ans1
|
|
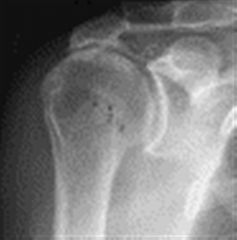
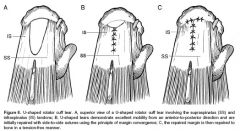
A 75-year-old, right-hand-dominant female has a chronic rotator cuff tear and shoulder pain for 10 years which has failed conservative treatment. A radiograph is shown in Figure A. Your examination and further imaging will help you to decide between which of the following pairs of surgical options for this patient? 1. hemiarthroplasty or total shoulder arthroplasty 2. reverse total shoulder or total shoulder arthroplasty 3. hemiarthroplasty or reverse total shoulder arthroplasty 4. total shoulder arthroplasty or glenohumeral arthrodesis 5. total shoulder arthroplasty or scapulothoracic arthrodesis
|
The radiograph shows superior migration of the humeral head with significant glenohumeral degenerative joint disease suggestive of rotator cuff arthropathy. Rotator cuff arthropathy is characterized by bony erosion, superior migration of the humeral head, and erosion of the acromion and acromioclavicular joint. The results of total shoulder arthroplasty performed as management for rotator cuff arthropathy had been disappointing due to poor function, continued superior migration, and glenoid component loosening ("rocking horse" phenomenon). Two better options are humeral head replacement (hemiarthroplasty) or reverse total shoulder arthroplasty (R-TSA). Hemiarthroplasty was a popular choice prior to the development of the reverse. Zuckerman et al showed improved pain scores and mild functional improvements in a small case series. Leung recently showed better results for the R-TSA than for hemi in their patients. A hemiarthroplasty may still be preferred if their is insufficient glenoid bone stock or poorly functioning deltoid which you cannot rule out based on this single radiograph. Gerber discusses the development of the R-TSA but notes that is has a significantly higher complication rate than conventional arthroplasty.Ans3
|
|
|
Which patient has the best indication for latissimus dorsi transfer? 1. 55-year-old man with cuff tear arthropathy and proximal humeral migration 2. 85-year-old man with irreparable posterosuperior rotator cuff tear and 60 degrees of forward elevation and 0 degrees of active external rotation at his side 3. 45-year–old man with complete irreparable supraspinatus and subscapularis tears with 90 degrees of active forward elevation 4. 50-year-old man with large irreparable posterosuperior rotator cuff tear with 100 degrees of forward elevation and -10 degrees of external rotation 5. 35-year-old with an acute traumatic complete posterosuperior cuff tear with 0 degrees of active external rotation
|
The best indication for latissimus dorsi tendon transfer is a younger adult patient with an irreparable posterosuperior rotator cuff tear, lack of advanced glenohumeral arthritis, has an intact subscapularis function to stabilize the humeral head after latissimus transfer, and who maintains some active forward elevation. Gerber demonstrated that a dysfunctional subscapularis is a relative contraindication as those patients without a subscapularis did poorly. The functional value of subscapularis deficient shoulders valued only 48% clinically while those with intact subscapularis were at 84%. Incorrect Answers:Answer 1: Cuff tear arthropathy may continue to be painful after a latissimus dorsi transfer.Answer 2: An elderly patient >80 with a pseudoparalytic shoulder may not regain enough strength from a latissimus dorsi transfer.Answer 3: A deficient subscapularis has poor results after latissimus transfer likely because of imbalance and instability.Answer 5: An acute cuff tear in a young patient should have an attempted repair prior to any transfer.Ans4
|
|
|
What is the average medial-to-lateral distance of the supraspinatus tendon insertion at its footprint on the greater tuberosity? 1. 6-8mm 2. 14-16mm 3. 20-22mm 4. 24-26mm 5. 30-32mm
|
Cadaveric studies have shown the average medial-to-lateral distance of the supraspinatus tendon footprint on the greater tuberosity is 14-16mm.Curtis et al dissected 20 fresh-frozen cadavers in order to identify the length and width of each rotator cuff muscle insertion on the humerus. They found that the average maximum insertional length (anterior to posterior distance, distance Y in Illustration A) and width (medial to lateral distance, distance X in Illustration A) of the supraspinatus insertion was 23 x 16mm respectively. Ans2
|
|
|
A latissimus dorsi tendon transfer is a well established procedure for treatment of massive irreparable posterosuperior rotator cuff tears. All of the following factors have been shown to result in worse clinical outcomes after a transfer EXCEPT? 1. Nonsynergistic action of the transferred muscle 2. Fatty atrophy of the supraspinatus and infraspinatus 3. Deficiency of the subscapularis 4. Absence of the coracoacromial ligament 5. Deltoid weakness
|
A latissimus dorsi tendon transfer can be utilized in patients with a massive, irreperable rotator cuff tear involving the supraspinatus and infraspinatus. It has been reported to relieve pain and improve function in a carefully selected patient population. Those patients with deficiency of the deltoid or subscapularis, nonsynergistic muscle action after transfer, or fatty infiltration of the posterosuperior cuff have worse clinical outcomes. Absence of the CA ligament may allow anterosuperior escape in RC deficient shoulders but has not been shown to lead to worse outcomes after a tendon transfer. The paper by Warner, et. al demonstrated that poor tendon quality, stage 3/4 muscle fatty degeneration, and detachment of the deltoid insertion each had a statistically significant effect on the Constant score noting that salvage reconstruction of a previous cuff repair had more limited gains as compared to primary. The reference by Ianotti, et. al showed that synchronous in-phase contraction of the transferred latissimus dorsi is associated with a better clinical result while improved preoperative shoulder function and general strength also positively influence the clinical result.Ans4
|
|

A 30-year-old male sustains a right shoulder injury with initial radiographs shown in Figures A and B. What single piece of additional information would best assist in determining this patient's functional outcome? 1. Lower extremity injury 2. Neurological deficit 3. Contralateral upper extremity injury 4. Proximal humerus fracture 5. Worker's compensation
|
Figures A and B show a scapulothoracic dissociation, with significant lateralization of the scapula and widening of the acromioclavicular joint to over 4 cm (Figure A). This can be thought of as an internal disarticulation of the scapulothoracic association and acromioclavicular joints.Ans2
|
|
|
A patient presenting with scapulothoracic dissocation and ipsilateral extremity neurologic injury is most likely to have which of the following outcomes? 1. Glenohumeral arthritis 2. Return of 3/5 motor strength in distal extremity 3. Full return of extremity sensory function only 4. Flail extremity 5. Death
|
Scapulothoracic dissociation is a high-energy injury resulting from massive traction injury to the shoulder girdle with disruption of the scapulothoracic articulation. The most common long term result from this injury is complete loss of motor and sensory function of the extremity (flail limb), with death in the acute or semi-acute period also common. Ans4
|
|
|
A 23-year-old professional pitcher complains of posterior shoulder pain. Physical exam is notable for scapular dyskinesis. No intra-articular pathology is found on shoulder MRI. Which of the following should be emphasized in the initial stages of rehabilitation? 1. Isometric shoulder exercises 2. Isokinetic shoulder exercises 3. Closed chain shoulder exercises 4. Coordination of scapular motion with trunk and hip movements 5. Axial loading shoulder exercises
|
Scapular dyskinesis is an alteration in the normal motion of the scapula during coordinated scapulohumeral movements. It occurs as a sequela of prior shoulder injury, especially injuries disrupting the activation patterns of scapular stabilizing muscles. Kibler et. al outlined a rehabilitation protocol to treat scapular dyskinesis. The principle is to treat the problem from proximal to distal. The first stage involves attaining full motion of the scapula and coordinating the scapula with trunk and hip motions. Once this has been achieved, the second stage involves strengthening the scapular musculature. As scapular control is attained, exercises are introduced that place emphasis on the shoulder and arm beginning with flexibility and closed-chain strengthening, and eventually working up to sport-specific functions. Progress is determined by functional improvement rather than a strict time table. Kibler et al outline the presentation, evaluation, and treatment for scapular dyskinesis in the JAAOS review article. They specifically discuss the acute, recovery, and maintenance phases of rehabilitation.Ans4
|
|
|
|
|
|
|
|
|
patient has pain with overhead activities and night pain with the diagnosis |
rotator cuff tear |
|
|
what physical exam finding confirmed teres minor tear |
Hornblower sign External rotation weakness at 90° abduction and 90° it is excellent rotation |
|
|
the patient has weakness with internal rotation and 0° abduction and a positive belly press with diagnosis |
subscapularis tear |
|
|
patient complains of weakness in external rotation at 0° abduction and has an external lag sign once the diagnosis |
infraspinatus tear |
|
what the diagnosis |
biceps tendon subluxation = subscapularis tear |
|
|
what are the indications for a rotator cuff tear repair |
|
|
|
with a rate limiting step or recovery after rotator cuff repair |
biologic healing of the rotator cuff tendon to the greater tuberosity which takes approximately 8–12 weeks |
|
|
once the surgical treatment of a massive rotator cuff tear |
latissimus dorsi transfer with an intact subscapularis |
|
|
with the treatment for a chronic subscapularis tear |
pectoralis major transfer |
|
|
with the treatment for large supraspinatus and infraspinatus tear and a young healthy laborer |
latissimus dorsi transfer |
|
|
most comminuted organism to cause delayed infection and rotator cuff repair |
Propionibacterium acnes |
|
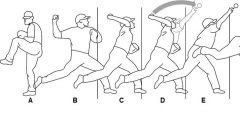
The rotator cuff in an overhead throwing athlete is most susceptible to tensile failure due to eccentric loading during which of the phases of throwing shown in Figure A? 1. A 2. B 3. C 4. D 5. E |
Label E is the deceleration phase of throwing in the overhead athlete. During this phase of throwing, the rotator cuff is the principal decelerator of the arm. The rotator cuff is susceptible to tensile failure due to eccentric loading during this phase. In throwers, these tears often occur on the articular side of the posterior supraspinatus or the infraspinatus. They may complain of posterior shoulder pain that is worse after ball release. ans5 |
|
|
Which patient has the best indication for latissimus dorsi transfer? 1. 55-year-old man with cuff tear arthropathy and proximal humeral migration 2. 85-year-old man with irreparable posterosuperior rotator cuff tear and 60 degrees of forward elevation and 0 degrees of active external rotation at his side 3. 45-year–old man with complete irreparable supraspinatus and subscapularis tears with 90 degrees of active forward elevation 4. 50-year-old man with large irreparable posterosuperior rotator cuff tear with 100 degrees of forward elevation and -10 degrees of external rotation 5. 35-year-old with an acute traumatic complete posterosuperior cuff tear with 0 degrees of active external rotation |
The best indication for latissimus dorsi tendon transfer is a younger adult patient with an irreparable posterosuperior rotator cuff tear, lack of advanced glenohumeral arthritis, has an intact subscapularis function to stabilize the humeral head after latissimus transfer, and who maintains some active forward elevation. Gerber demonstrated that a dysfunctional subscapularis is a relative contraindication as those patients without a subscapularis did poorly. The functional value of subscapularis deficient shoulders valued only 48% clinically while those with intact subscapularis were at 84%. ans4 |
|
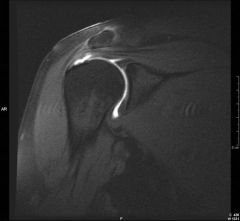
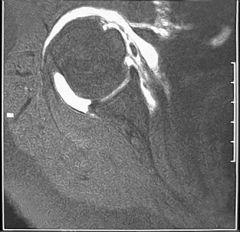
A 55-year-old carpenter presents with 6 weeks of right shoulder pain after installing ceiling drywall. He has no symptoms of night pain. His examination reveals 30 degrees lack of full flexion and abduction. He has full strength of the right shoulder. Radiographs are shown in Figures A and B. Coronal and Abduction-external rotation (ABER) MR images are shown in Figures C-E. What is the next most appropriate stem in management? 1. Physical therapy 2. Platelet rich plasma (PRP) injection 3. Arthroscopic rotator cuff repair 4. Arthroscopic SLAP repair 5. Arthroscopic subacromial decompression |
partial articular-sided supraspinatus tendon avulsion (PASTA). Physical therapy including shoulder range of motion and rotator cuff/periscapular stabilizer strengthening is the most appropriate initial treatment for the options provided.ans1 |
|
|
what is what is the prevalence of a symptomatic rotator cuff tear as diagnosed by MRI or ultrasound and patient's over the age of 60 |
MRI=54% one fourth full-thickness and a quarter were partial thickness Ultrasound greater than 30% |
|
|
Rotator cuff tears (full thickness and partial thickness) in asymptomatic individuals are seen on MRI or ultrasound in what percentage of patients over the age of 60? 1. 0-5% 2. 5-30% 3. 30-55% 4. 55-80% 5. 80-100% |
The prevalence of asymptomatic rotator cuff tears diagnosed with MRI or ultrasound is quite high, with most studies noting tears in 30-54% of patients over the age of 60. The paper by Tempelhof et al utilized ultrasound and found tears in 30% of patients over 60. The study by Sher et al noted an overall prevalence of 54% on MRI in patients older than 60 (28% had full thickness and 26% with partial thickness). In both studies the frequency of tears increased substantially with increasing age. ans3 |
|
|
During shoulder arthroscopy of a 58-year-old female recreational golfer, the rotator cuff is examined and is seen to be intact on the articular side. After a bursectomy is performed in the subacromial space, a bursal sided tear is found measuring 1.5 cm in width and 4 mm in depth with surrounding cuff softening. What is the appropriate management? 1. Debride the tear and perform an acromioplasty 2. Abort surgery and start a physical therapy program 3. Convert it to a full-thickness tear and repair it with suture anchors 4. Consider it incidental, as this is a common finding in this age group 5. Perform acromioplasty only |
Partial thickness rotator cuff tears on the articular side are more common than their bursal counterparts; however, the bursal tears are typically more symptomatic. Grading is based on depth (<25 |
|
|
What is the average medial-to-lateral distance of the supraspinatus tendon insertion at its footprint on the greater tuberosity? Review Topic QID: 3290
1. 6-8mm 2. 14-16mm 3. 20-22mm 4. 24-26mm 5. 30-32mm
|
Cadaveric studies have shown the average medial-to-lateral distance of the supraspinatus tendon footprint on the greater tuberosity is 14-16mm. |
|
|
Which of the following may be seen during arthroscopy in a patient with a subscapularis tear? 1. Uncovered lesser tuberosity 2. Retraction of the subscapularis tendon to the level of the glenoid 3. Avulsed superior glenohumeral ligament 4. Medial biceps subluxation 5. All of the above |
Degenerative subscapularis tears often involve only the superior portions of the tendon. However, completely retracted tears also occur especially those occuring after trauma or previous surgery. All of the findings mentioned may be encountered. |
|
|
A 66-year-old male is undergoing a total knee arthroplasty using a fixed bearing posterior stabilized component. During intraoperative trialing of the components it is noted that the flexion gap is loose, and extension gap is appropriate. If this is not corrected, what post-operative complication is this patient at risk of having? 1. Spin out of the polyethylene 2. Periprosthetic fracture 3. Posterior knee dislocation 4. Osteolysis 5. Patellar instability |
A posteriorly stabilized knee has a post built into the polyethylene bearing that articulates with the box of the femoral component in flexion to act as a cam mechanism. If the knee is too loose in flexion, it is possible for the femoral component to "jump the post", causing a posterior dislocation. ans3 |
|
|
When performing a total knee arthroplasty, the knee is stable at full extension, but it will not flex past 90 degrees. Which of the following adjustments can achieve satisfactory range of motion and stability in flexion and extension? 1. Downsizing the tibial insert 2. Placing posterior femoral augments 3. Resecting more distal femur 4. Downsizing the femoral component 5. Performing a medial tibial reduction osteotomy
|
Balancing flexion and extension gaps in knee arthroplasty can be a challenge, especially in a revision setting. For a TKA to achieve greater flexion, options include downsizing the femoral component, recessing the PCL, and increasing the posterior tibial slope. More flexion can also be achieved by resecting more tibia or decreasing the height of the tibial insert; however, changes to the tibial side affect both the flexion and extension gaps. With regards to this question, downsizing the tibial insert would increase both the flexion and extension gaps; the knee would be unstable in extension. Placing augments on the posterior femur would make the flexion gap even tighter. Resection of more distal femur would loosen the extension gap without changing flexion. Tibial reduction osteotomy on the medial side would result in more laxity to valgus stress, but it would not symmetrically increase the flexion gap. The paper by Dennis et al. is a review of revision knee arthroplasty, in which there is complete discussion of gap balancing techniques. The technique paper by Ries et al. covers only balancing in revision total knee arthroplasty. ans4 |
|
|
|
|
|
what area of the scaphoid has 100% AVN Rate |
proximal 5th |
|
|
with the major blood supply to the scaphoid |
dorsal carpal branch of the radial artery |
|
|
patient presents to the office after slip and fall physical exam demonstrates anatomic snuffbox tenderness dorsally
|
|
|
|
|
|
|
fixation rigidity is most optimized by what technique |
locking screw down the central axis of the scaphoid |
|
|
what additional procedure should be done if there is evidence of impaction osteoarthritis between the radial styloid and the scaphoid |
radial styloidectomy |
|

|
|
|

A 30-year-old female reports 5 months of wrist pain after a fall onto her wrist. A radiograph is shown in Figure A. If untreated, all of the following degenerative changes may be observed EXCEPT? 1. radial styloid osteophyte 2. radioscaphoid arthritis 3. midcarpal arthritis 4. scapholunate arthritis 5. radiolunate arthritis |
Radiographs show a scaphoid non-union which can lead to Scaphoid Nonunion Advanced Collapse (SNAC wrist) and progressive arthritis. The natural history of degenerative changes first occurs at the radioscaphoid area and progresses to pancarpal arthritis. All of the answers above are features of a SNAC wrist except radiolunate arthritis. ans5 |
|
|
|
|

|
|
|
|
hereditary VITAMIN D dependent rickets type I and 2
|
|
|
|
|
|
|
Laboratory values of a normal serum calcium and parathyroid hormone can be found in which of the following disease states? 1. Primary hyperparathyroidism 2. Type I vitamin D deficient rickets 3. Type II vitamin D deficient rickets 4. X-linked hypophosphatemic rickets 5. Nutritional rickets |
Hypophosphatemic rickets is caused by the inability of kidney proximal tubules to reabsorb phosphate due to a mutated PHEX gene, found on the X chromosome. PHEX is thought to protect extracellular matrix glycoproteins from proteolysis. Hypophosphatemic rickets shares many clinical similarities with nutritional rickets but shows PTH levels that are not elevated, even with calcium and phosphate abnormalities. ans4 |
|
|
|
|
patient involving motor vehicle accident presents with peripelvic pain
|
|
|

|
|
|

|
|
|

what is the most stable construct for fixation for an unstable transforaminal sacral fracture |
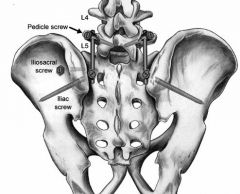
iliosacral and lumbopelvic fixation triangular osteosynthesis |
|
|
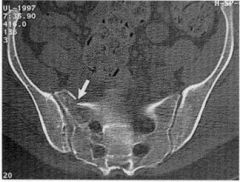
Which of the following is the most stable construct for fixation of an unstable transforaminal sacral fractures? 1. External fixation 2. Iliosacral osteosynthesis 3. Combined iliosacral and lumbopelvic fixation (triangular osteosynthesis) 4. Anterior pelvic ring plating with bilateral sacroilliac percutaenous screw fixation 5. Transiliac bars with anterior pelvic ring plating |

Combined iliosacral and lumbopelvic fixation (triangular osteosynthesis) for sacral fractures has the greatest stiffness when used for an unstable sacral fracture. |
|

patient presents with pseudoparalysis of the shoulder pain subjective weakness
|
|
|
|
|
|
|
what is the requirement for reverse total shoulder prosthesis |
|
|
|
risk factors for rotator cuff arthropathy |
|
|
|
which physical exam test confirmed teres minor dysfunction |
Hornblower sign |
|
|
which physical exam test confirmed infraspinatus tear |
external rotation lag sign |
|

patient presents with history of high energy trauma and pain and numbness and tingling involving the entire upper extremity
|
|
|
|
|
|
|
A 60-year-old woman with rheumatoid arthritis has long term neck pain and new onset of difficulty holding cards in her weekly poker tournament. She does not complain of weakness, but states she has become "clumsy" in her old age, fumbling with buttons and dropping her change. On exam she has hyperreflexia, but no weakness. Radiographs show atlantoaxial subluxation. She is considering decompressive surgery, but wants to know if she will recover function. Which radiographic marker may predict neural recovery after decompression? 1. Posterior atlanto-dens interval of >13mm 2. Atlanto-dens interval of <5mm 3. Subaxial subluxation of <3.5mm 4. Basilar invagination <0.5cm 5. Rotary subluxation of <10 degrees
|
The clinical presentation is consistent for cervical myelopathy due to atlantoaxial subluxation in a patient with rheumatoid arthritits. |
|
|
what is the single most important marker for neurologic recovery with atlantoaxial subluxation |
posterior atlantoodontoid interval >10 mm if posterior atlantoodontoid interval<10 there was no neurologic recovery |
|

Child presents to the clinic with a diet of condensed milk with fatigue
|
|
|
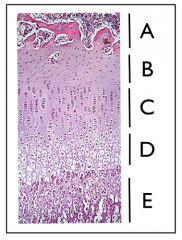
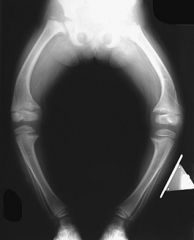
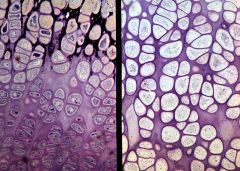
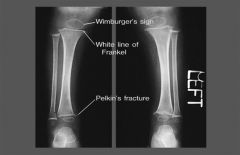
A 7-year-old recent immigrant presents with pain and tenderness over the legs. Physical exam shows the gums have a bluish-purple hue with areas of hemorrhages. A radiograph is shown in Figure A. In Figure B, what region of the growth plate is most affected in this condition? 1. A 2. B 3. C 4. D 5. E |
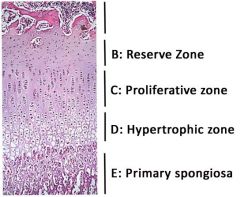
The clinical presentation and radiographs are consistent with scurvy. The radiographs show a dense band (White line of Frankl) at the growing metaphyseal end which is characteristic of Scury. Scurvy is a disease resulting from a deficiencyans5 of vitamin C (ascorbic acid), which is required for the synthesis of collagen in humans. Impaired collagen synthesis in scurvy leads to fragile capillaries, resulting in abnormal bleeding, and altered bone formation at the growth plate. More specifically, scurvy affects the spongiosa the most (but not exclusively) in the metaphysis, which is depicted by region E in the illustration.
|
|
patient presents with this out as Omaha inheritance pattern and is concerned about how he looks
|
|
|
|
A 23-year-old professional pitcher complains of posterior shoulder pain. Physical exam is notable for scapular dyskinesis. No intra-articular pathology is found on shoulder MRI. Which of the following should be emphasized in the initial stages of rehabilitation? 1. Isometric shoulder exercises 2. Isokinetic shoulder exercises 3. Closed chain shoulder exercises 4. Coordination of scapular motion with trunk and hip movements 5. Axial loading shoulder exercises |
Scapular dyskinesis is an alteration in the normal motion of the scapula during coordinated scapulohumeral movements. It occurs as a sequela of prior shoulder injury, especially injuries disrupting the activation patterns of scapular stabilizing muscles. Kibler et. al outlined a rehabilitation protocol to treat scapular dyskinesis. The principle is to treat the problem from proximal to distal. The first stage involves attaining full motion of the scapula and coordinating the scapula with trunk and hip motions. Once this has been achieved, the second stage involves strengthening the scapular musculature. As scapular control is attained, exercises are introduced that place emphasis on the shoulder and arm beginning with flexibility and closed-chain strengthening, and eventually working up to sport-specific functions. Progress is determined by functional improvement rather than a strict time table. Kibler et al outline the presentation, evaluation, and treatment for scapular dyskinesis in the JAAOS review article. They specifically discuss the acute, recovery, and maintenance phases of rehabilitation. |