Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
Functions of bile.
|
Lipid digestion
Disposal of hphobic materials Aids in absorption of fat soluble vits |
|
|
Synthesis of bile acid. Begin with cholesterol, end with a bile salt.
|
Cholesterol-->CholylCoA-->Cholic Acid/Chenodeoxycholic acid (primary bile acids)
Cholic acid-->deoxycholic acid (secondary bile acid; via bacteria) Chenodeoxycholic acid-->lithocholic acid (secondary bile acid; via bacteria) -->within liver, conjugated to glycine or taurine before being re-secreted (in gut, glycine/taurine removed)-->glychocholic/taurocholic acid |
|
|
Why must bile acids be conjugated before their secretion?
|
Conjugation to glycine/taurine improves hydrophilicity (lose less bile acid this way)
|
|
|
Describe location of bile during:
Fasting state Beginning of meal After a meal |
Fasting: bile acid moves down biliary tract and concentrated in gallbladder (low levels of bile acids in small intestine, portal vein, liver)
Meal-->CCK released from intestinal mucosa-->relax sphincter of Oddi, stimulates gallbladder. Bile acids flow into intestines. GB remains contracted, bile acids secreted by liver bypass gallbladder and go directly to duodenum. After meal: SOD contracts, gallbladder relaxes and begins to fill. |
|
|
Gall stones are highly prevalent in this population.
|
Pima Indians
|
|
|
How are stones formed?
|
Motility: gall bladder not contracting well-->gall bladder stasis-->stone formation
Nucleation Factors(...) Supersaturation of Bile w/cholesterol: supersaturation of cholesterol-->more potential for crystal formation |
|
|
Risk factors for gallstones.
|
Sex (women!)
Race, weight, age PREGNANCY OCPs (estrogen!) Rapid weight loss (gastric bypass) Cirrhosis TPN (gallbladder stasis) |
|
|
Why is pregnancy a risk for gallstones?
|
Supersaturation due to E2-induced increase in cholesterol secretion and Progest-induced reduction in BA secretion
Overproduction of hphobic bile acids-->reduced ability to solubilize cholesterol Progesterone-induced slowing of gall bladder emptying. |
|
|
Cholesterol gallstones:
Composition Color Location |
50-100% cholesterol
Yellow-brown Location: gallbladder +/- common duct |
|
|
Cholodocolithiasis:
What is it? |
Gall stone stuck in common bile duct
|
|
|
Black Pigment Stones:
Composition Color Location |
Calcium bilirubinate polymer
Black Gallbladder +/- common duct Seen with anyone who has RBC destruction |
|
|
Brown Pigment Stones:
Composition Color Location |
Unconj'd bilirubin, calcium soaps
Brown Bile ducts Seen in pts with infection/inflammn |
|
|
This stone is seen in patients with increased RBC destruction.
|
Black pigment
|
|
|
This stone is seen in patients with metabolic derangement.
|
Cholesterol gallstone
Metabolic derangement = obestiy, +famhx, aging (excessive chol secretion), women |
|
|
This stone is seen in patients with infections.
|
Brown pigment
|
|
|
Biliary colic:
Presentation Cause Labs Dx Tx |
Severe, localized RUQ pain
Due to intermittent obstruction of cystic duct Note: 30% asyx Labs: nl Dx: Ultrasound along w/clinical hx Tx: Cholecystectomy |
|
|
Ursodeoxycholic acid:
Effects Indication |
Mech unknown but:
-inhibits biliary secretion of cholesterol -increases hepatic bile secreiton -inhibits deposition of cholesterol into stones -improves gallbladder emptying -improves gallbladder muscle contractility -reduces gallbladder inflammn Indication: Pts w/small gallstones sans calcification |
|
|
Acute Cholecystitis:
Presentation Cause Labs Dx Tx |
Severe, localized pain in RUQ with n/v/f
Causes: impacted stone in cystic duct, acute inflammn of gallbladder mucosa, secondary bacterial infection Labs: Elevated WBCs, bilirubin, ALT/AST Dx: U/S, hepatobiliary scintigraphy (HIDA)--gallbladder doesn't light up! Tx: Abx, sx |
|
|
Murphy's Sign:
What is it? Indicative of? |
Upon palpation, right subcostal tenderness and inspiratory arrest (can't inspire when palpate!)
Indicates acute cholecystitis |
|
|
Choledocholithiasis:
Presentation Cause Labs Dx Tx |
Often asyx, but can present ~biliary colic; can see painless jaundice or RUQ tenderness
Due to obstruction of common bile duct Labs: elevated bilirubin, ALP Dx: U/S, MRCP (specialized MRI) Tx: ERCP (snip common bile duct and remove stones) |
|
|
Cholangitis:
Presentation Cause Tx |
Pain, jaundice, fever;
mental confusion, lethargy, delirium Cause: impacted stone in common bile duct-->bile stasis-->bacterial superinfection of stagnant bile Tx: Bile duct decompression (ERCP) |
|
|
Risk factors for developing gallbladder cancer.
|
Porcelain gallbladder (intramural calcification of gallbladder wall)
Gallbladder polyps Salmonella infection Biliary cysts |
|
|
Medical term for gallstone.
|
Cholelithiasis
|
|
|
Cholangiocarcinoma:
What is it? Risks of developing it |
Cancer of bile ducts
Risks: Primary sclerosing cholangitis Parasitic infection |
|
|
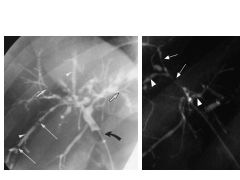
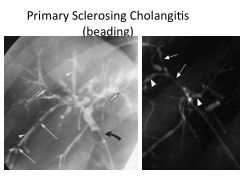
Primary Sclerosing Cholangitis:
What is it? Associated with? |
Progressive inflammation, stricturing, and fibrosis of bile ducts.
Associated with IBD, esp UC. Appears as beading. |
|
|
|